Hepatopulmonary Fascioliasis Presenting with Lung Abscess: A Case Report and Literature Review

Abstract
Introduction: Fascioliasis is a rare food-borne parasitic infection primarily of the hepatobiliary system caused by Fasciola hepatica. The liver is the principal site of infection, and involvement of other organs is infrequent. This report presents a rare case of fascioliasis associated with a lung abscess.
Case presentation: A 37-year-old female presented with abdominal pain and hematochezia. General examination was normal. Computed tomography (CT) scan showed multiple hypodense liver lesions with peripheral enhancement, with moderate left pleural effusion and a left lower lobe cavitary lesion. Ultrasonography (US) showed cystic liver lesions with curvilinear tracts. She underwent VATS (Video-assisted thoracic surgery) wedge resection of the left lower lobe cavitary lesion. She then received triclabendazole (TCBZ). Follow-up US showed new liver lesions, so a second course of TCBZ was given. Subsequently, the patient improved and was asymptomatic at the last follow-up.
Literature review: A review of seven reported cases of fascioliasis between 2013 and 2024 was performed, of which only two cases had pulmonary involvement. Five patients were females (71.43%), with a mean age of approximately 45 years (range: late 20s-58 years). The most prevalent presentation was fever in five cases (71.43%). Eosinophilia was present in six cases (85.71%). On clinical examination, abdominal tenderness was noted in three patients (42.86%). Management was exclusively conservative in six cases (85.71%).
Conclusion: This report highlights the diagnostic challenges of fascioliasis with extrahepatic involvement. Pulmonary findings require careful evaluation, and clinicians should maintain a high index of suspicion for ectopic fascioliasis, even without definitive parasitological confirmation.
Introduction
Fascioliasis is a rare food-borne parasitic infection affecting primarily the hepatobiliary system, caused by the digenean flatworms, Fasciola hepatica (F. hepatica) or Fasciola gigantica (F. gigantica), commonly known as liver flukes [1,2]. Fasciola gigantica is predominantly found in tropical regions, whereas F. hepatica thrives in temperate climates. Both species parasitize a wide range of herbivorous animals, with their larval stages residing on aquatic plants. Human infection most frequently occurs through the consumption of vegetation, such as watercress, that has been contaminated with metacercariae [1]. Cattle and sheep serve as the primary definitive hosts, placing individuals in livestock farming communities and those consuming raw aquatic vegetation at the greatest risk [1,2]. The main risk factors for human infection include ingestion of contaminated plants or water and consumption of undercooked infected animal liver [3]. Ectopic fascioliasis is an infection occurring outside the hepatobiliary system [1]. Although F. hepatica predominantly affects the liver, involvement of other organs has been documented in rare instances [4]. Pulmonary involvement, including lung abscess formation, represents a rare ectopic manifestation [5].
This report presents a rare case of fascioliasis with pulmonary manifestation. The report was prepared in accordance with the CaReL guidelines, and all referenced sources were critically assessed for reliability [6,7]
Case presentation
Patient information
A 37-year-old female presented with abdominal pain for three months, mainly postprandial epigastric pain, associated with weight loss. She also had occasional hematochezia and night sweats, along with a one-week history of hemoptysis. There was no travel history. There was a history of heavy consumption of watercress (Nasturtium officinale). Past medical history included a possible thrombotic event during pregnancy.
Clinical findings
General examination was unremarkable. During the course of illness, she developed urticaria and an anaphylactic reaction characterized by shortness of breath, along with mild abdominal discomfort.
Diagnostic assessments
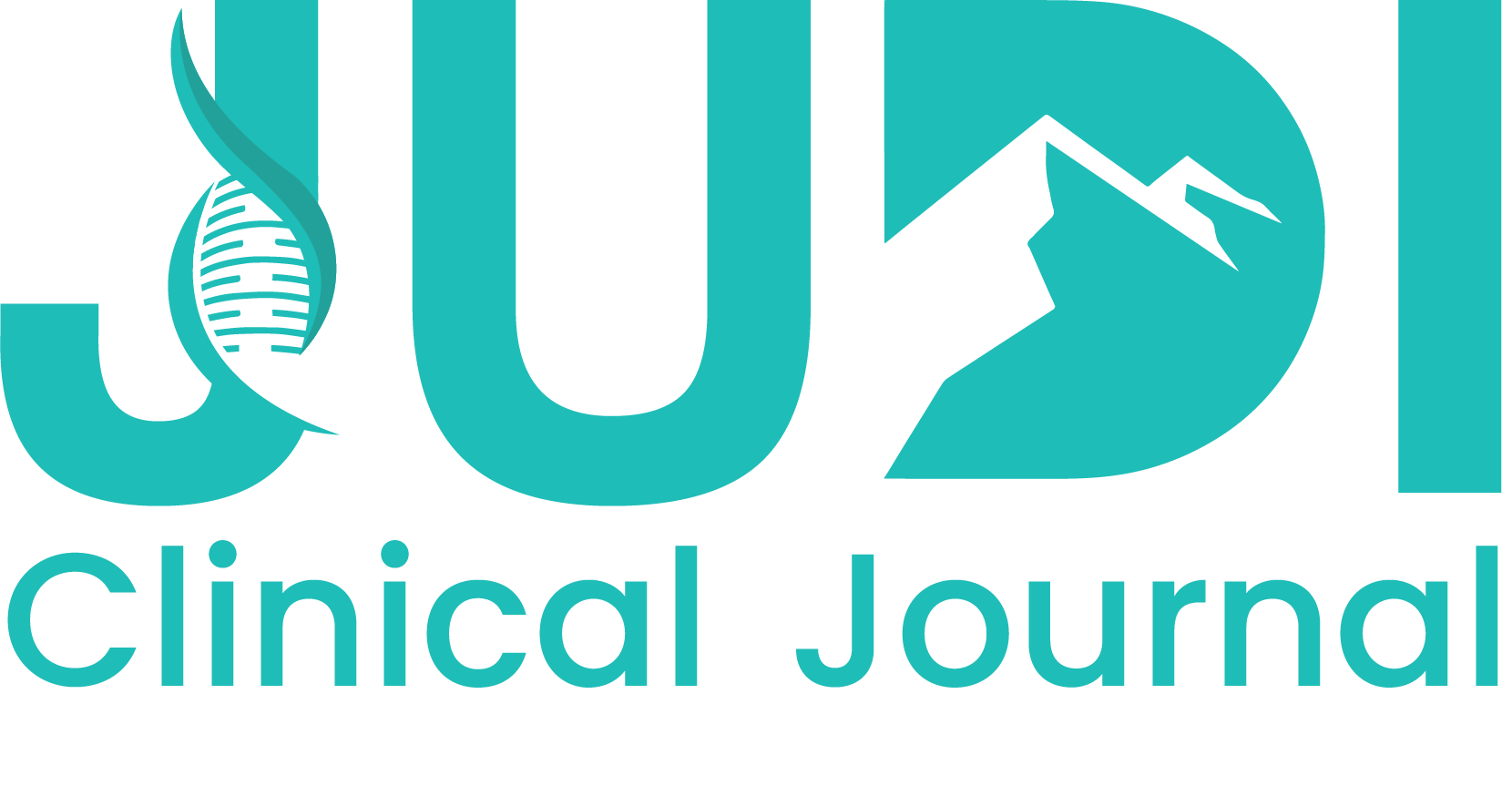
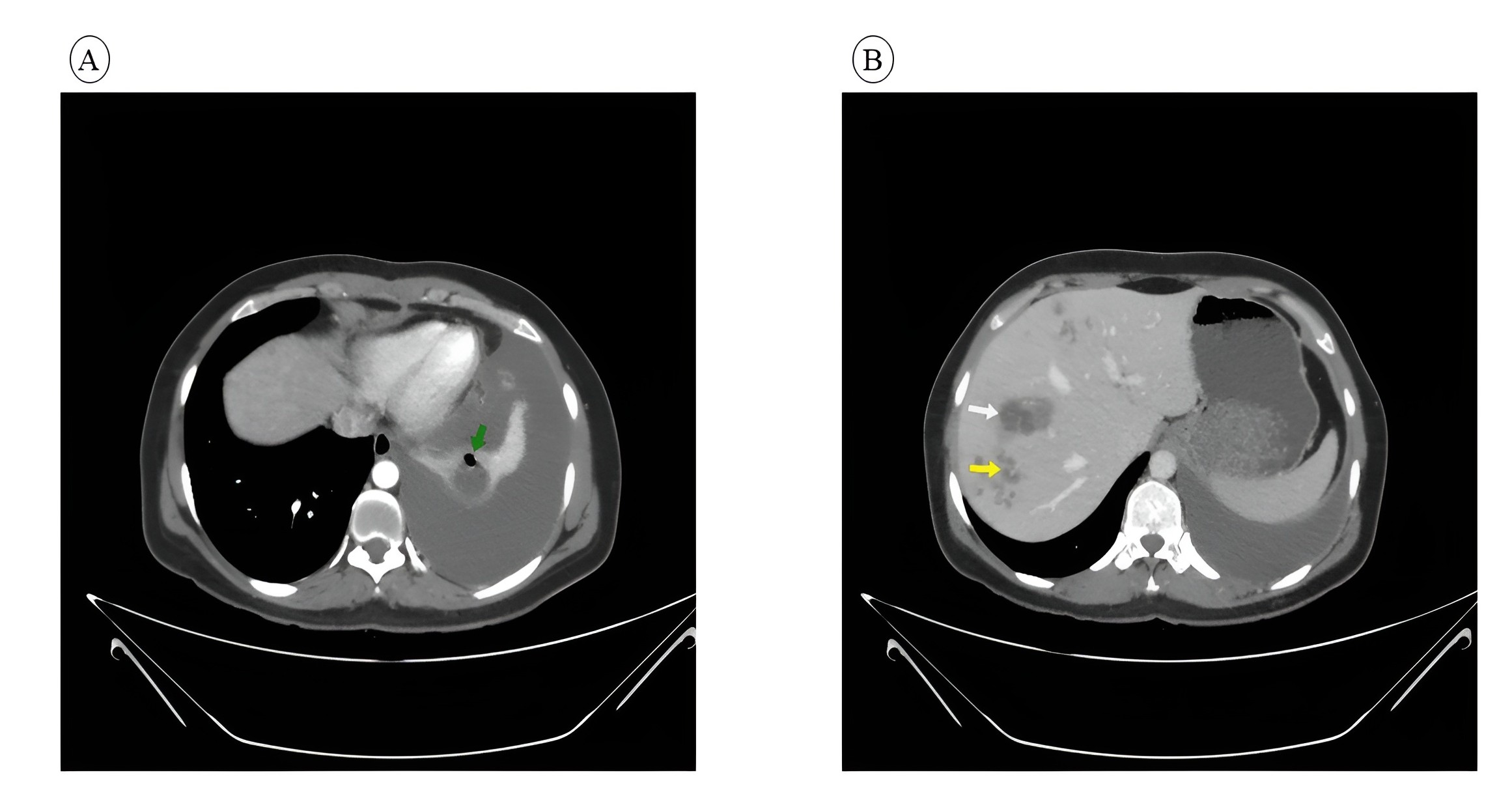
Laboratory investigations revealed leukocytosis 11.7 × 10^9/L (normal range: 3.4–9.6 ×10^9/L) and eosinophilia 13% (normal range: 1% to 6%), suggesting an active inflammatory or parasitic process. Thrombocytosis was also noted 494 x10^9/L (normal range: 157–371 ×10^9/L). Inflammatory and biochemical markers were elevated, including C-reactive protein (CRP) 16.9 mg/L (normal range: below 3.0 mg/L). Additionally, the CA-125 level was 55.0 U/mL (normal range: 0–35 U/mL). Renal function remained normal (Table 1). Computed Tomography (CT) scan of chest, abdomen, and pelvis showed multiple hypodense liver lesions with peripheral enhancement, suggestive of infection, mostly fascioliasis, with moderate left pleural effusion and a left lower lobe cavitary lesion suggestive of a lung abscess with possible rupture into the pleural space (Figure 1). Ultrasonography (US) showed cystic liver lesions with curvilinear tracts in keeping with fascioliasis. Fasciola hepatica serology was positive, while hydatid serology, pleural fluid culture, and the acid-fast bacilli tests were negative.
|
Test category |
Result |
Normal range |
|
WBC count |
11.7 × 10^9/L |
3.4–9.6 ×10^9/L |
|
Eosinophil |
13.00% |
1% to 6% |
|
Platelet |
494 × 10^9/L |
157–371 ×10^9/L |
|
Creatinine |
0.625 mg/dL |
0.6-1.1 mg/dL |
|
CRP |
16.9 mg/L |
below 3.0 mg/L |
|
LDH |
257 IU/L |
105–233 IU/L |
|
CA-125 |
55.0 U/mL |
0–35 U/mL |
|
WBC: White blood cell, CRP: C-reactive protein, LDH: Lactate dehydrogenase, CA: Cancer antigen |
||
Therapeutic intervention
Medical therapy was considered; however, due to the thick-walled nature of the lesion and the uncertainty regarding the underlying diagnosis, and the possibility of the condition not responding adequately to conservative treatment, surgical management was preferred. She underwent VATS (Video-assisted thoracic surgery) wedge resection of the left lower lobe cavitary lesion. Postoperatively, she was treated with triclabendazole (TCBZ). Histopathological examination of the lung wedge specimen demonstrated pyogenic necrotizing inflammation with abscess formation, no malignancy, and no identifiable Fasciola eggs, larvae, or parasites.
Follow-up and outcomes
Follow-up US showed new liver lesions consistent with ongoing fascioliasis, for which a second course of TCBZ was administered. At the two-week postoperative follow-up, the patient had improved and was asymptomatic.
Discussion
Fascioliasis presents with variable manifestations depending on the disease phase, with the chronic stage often being asymptomatic. It is frequently misdiagnosed as other hepatobiliary conditions, particularly metastatic liver disease [2]. Delayed or misdiagnosis is still frequent because the disease is rarely encountered in nonendemic areas and its clinical presentation is non-specific. The history of recent travel to endemic zones should be considered when consistent radiological findings are suggestive of infection [2]. Fascioliasis involves two distinct phases: an acute stage characterized by larval migration through the liver parenchyma, and a chronic phase where mature flukes reside in the bile ducts. These flukes can survive in the biliary ducts for many years and may cause biliary inflammation and/or obstruction [8]. In rare cases, the parasites may migrate beyond the hepatobiliary system and involve other organs, including the lungs, with F. hepatica more commonly associated with ectopic infection [5,9].
A review of the literature on Google Scholar was conducted. Seven reported cases from 2013 to 2024 were reviewed, of which only two cases had pulmonary involvement. Five patients were females (71.43%), and two were males (28.57%), with a mean age of approximately 45 years (range: late 20s-58 years). The most prevalent presentations were fever in five cases (71.43%) and abdominal pain in four cases (57.14%). Eosinophilia was present in six cases (85.71%). On clinical examination, abdominal tenderness was noted in three patients (42.86%). Imaging findings included US in three cases (42.86%), chest X-ray in two cases (28.57%), CT scan in five cases (71.43%), and MRI (magnetic resonance imaging) in four cases (57.14%). Management was exclusively conservative in six cases (85.71%), with one case combining conservative and surgical approaches (14.29%). Follow-up showed clinical improvement in five cases (71.43%), complete cure in one case (14.29%), and no available data in one case (14.29%) (Table 2) [2,3,5,8,10–12].
|
Author/Reference |
Year |
No. of Patients |
Sex |
Age |
Presentation |
Clinical findings |
Diagnostic Technique |
Management & Treatment |
Follow-up & Outcome |
|
Salahshour & Tajmalzai [2] |
2021 |
1 |
F |
35 |
RUQ pain, fever, fatigue, and anorexia. |
RUQ tenderness, eosinophilia, slightly raised CRP |
CT scan, MRI, and ELISA. |
TCBZ |
Clinical improvement |
|
Matin et al. [10] |
2022 |
1 |
F |
38 |
Fever, RUQ pain, chills, non-productive coughs, anorexia, and nausea |
Tenderness in the RUQ, eosinophilia |
US, CT scan, ELISA, biopsy |
TCBZ |
Complete resolution of symptoms |
|
Rinaldi et al. [3] |
2020 |
1 |
M |
58 |
Abdominal pain, nausea, anorexia, and jaundice. cold night sweats, weight loss, weakness |
Eosinophilia |
US, MRI, x-ray, colonoscopy, EGD, ELISA, and ERCP |
TCBZ and sphincterotomy |
Reduction in mass size; clinical improvement. |
|
Pinarlik et al. [11] |
2023 |
1 |
F |
57 |
Fever, nausea, vomiting, and weight loss |
Fever, RUQ tenderness, and eosinophilia. |
MRI, Biopsy, and ELISA |
TCBZ |
Regression of abscess at 12-month follow-ups |
|
Girma et al. [8] |
2024 |
1 |
M |
20s |
Chronic bilateral upper quadrant pain, nausea, loss of appetite, fatigue, intermittent fever, and weight loss |
Mildly elevated transaminases; no identified risk factors. |
US, CT, MRI , MRCP, and ELISA |
TCBZ |
N/A |
|
Musa et al. [5] |
2013 |
1 |
F |
56 |
Chest pain, Fever, chills, cough, and weight loss. |
Eosinophilia |
X-Ray, CT, and bronchoscopy |
TCBZ |
Clinically well at present. Serology was repeated after 2 months and |
|
Castillo et al. [12] |
2020 |
1 |
F |
25 |
diarrhea and bloating, fatigue, nighttime urticaria, and a nonproductive cough |
Eosinophilia |
CT, EGD, MRI, biopsy |
TCBZ |
clinical and radiographic resolution of liver lesions, improvement of eosinophilia |
|
M: Male, F: Female, RUQ: Right upper quadrant, CRP: C-reactive protein, CT: Computed tomography, MRI: Magnetic resonance imaging, ELISA: Enzyme-linked immunosorbent assay, TCBZ: Triclabendazole, US: Ultrasonography, ERCP: Endoscopic retrograde cholangiopancreatography, MRCP: Magnetic resonance cholangiopancreatography, EGD: Esophagogastroduodenoscopy |
|||||||||
Presentations of fascioliasis usually include eosinophilia, right hypochondrial pain, intermittent fever, cold night sweats, nausea, vomiting, loss of appetite, weight loss, and urticarial itching [2,8,11]. Eosinophilia is considered a hallmark feature of fascioliasis [5]. Eosinophilia might still be absent because it subsides after the immunologic response; instead, it is replaced with mild inflammation, which explains persisting fever, loss of appetite, and weight loss [11]. Lung abscess typically presents with fever, cough, dyspnea, and may be associated with hemoptysis [9]. Pulmonary changes such as infiltrates may arise indirectly due to a strong immunological response triggered during the early phases of Fasciola hepatica invasion and migration. Respiratory manifestations have been documented, but they are rare in fascioliasis [12]. In the present case, the patient presented with abdominal pain and eosinophilia, typical of fascioliasis. She also had occasional bright per-rectal bleeding and night sweats. Hemoptysis was also noted, potentially a sign of the associated lung abscess.
Diagnosis of fascioliasis can be done through direct parasitological and indirect immunological tests, as well as imaging modalities. Stool examination for eggs has traditionally been used but has limited sensitivity [3]. Imaging plays a key role in diagnosis. Characteristic findings include “tunnels and caves” reflecting fluke migration tracts [5]. Liver flukes produce microabscesses, resulting in hypoechoic nodules and cystic lesions on US, and nodular or linear hypodensities on CT, which enhance homogeneously with dye. While nodular lesions are non-specific, the linear tracks are diagnostic of fascioliasis [5,8]. Computed tomography scan may also demonstrate areas of necrosis, fibrosis, and subcapsular lesions [11]. Chest imaging, particularly CT, is essential for identifying pulmonary complications such as lung abscess [9,13]. In the current case, the diagnosis of fascioliasis was based on clinical features, positive serology, and characteristic imaging findings in the absence of direct parasitological confirmation. This highlights a diagnostic limitation in ectopic fascioliasis, where definitive identification of the parasite may not be feasible. Ectopic involvement of Fasciola in the pleura or lungs has also been difficult to confirm in a previous report [14]. A direct causal relationship with F. hepatica often cannot be definitively established, and the association may remain presumptive. Given the lack of direct parasitic visualization, alternative etiologies for the lung abscess were considered. A primary alternative is a standalone pyogenic bacterial lung abscess co-occurring with an unrelated hepatic process. However, the patient's pleural fluid cultures were negative, and the liver lesions demonstrated pathognomonic 'furrow signs' rather than the standard spherical appearance of typical pyogenic or amebic liver abscesses. Other regional pulmonary pathogens, such as Mycobacterium tuberculosis and Echinococcus granulosus, were explicitly ruled out via negative acid-fast bacilli testing and negative hydatid serology, respectively. Additionally, histopathological evaluation of the resected lung tissue ruled out underlying malignancy.
Triclabendazole is the treatment of choice for fascioliasis [12]. It is effective against both immature and adult parasites, making it suitable for both acute and chronic phases [9]. Treatment typically consists of one to two oral doses, achieving high cure rates, although repeat dosing may be required in refractory cases [1,5,9]. F. hepatica is resistant to praziquantel [3], and alternative agents such as bithionol and nitazoxanide may be considered in selected cases [1,3,9]. Empiric antibiotic therapy should be considered when a lung abscess is suspected. Larger lung abscesses are less likely to respond to antibiotics alone and may necessitate surgical management, such as lobectomy [9]. In the reported case, the patient underwent VATS wedge resection of the left lower lobe cavitary lesion. Follow-up US demonstrated persistent hepatic lesions, for which a second course of TCBZ was administered.
During follow-up, several parameters should be assessed, including resolution of eosinophilia, absence of eggs in stool samples, decreasing serologic titers, and overall clinical improvement. In addition, normalization of biliary tract abnormalities on US can offer important information [3]. Prognosis is excellent once the diagnosis of fascioliasis is made [1]. In most cases, empiric antibiotic therapy successfully treats primary lung abscesses [9]. In this case, follow-up US showed new liver lesions consistent with ongoing fascioliasis, for which a second course of TCBZ was administered. Subsequently, the patient improved and was asymptomatic at the last follow-up.
Our report has several limitations. Definitive parasitological confirmation was not achieved, and no causative organism for the lung abscess was identified. In addition, a short follow-up limited assessment of long-term outcomes.
Conclusion
This report highlights the diagnostic challenges of fascioliasis with extrahepatic involvement. Pulmonary findings require careful evaluation, and clinicians should maintain a high index of suspicion for ectopic fascioliasis, even without definitive parasitological confirmation.
Declarations
Conflicts of interest: The authors have no conflicts of interest to disclose.
Ethical approval: Not applicable.
Consent for participation: Not applicable.
Consent for publication: Informed consent was obtained from the patient for the publication of the present and any accompanying images.
Funding: The present study received no financial support.
Acknowledgments: None to be declared.
Authors' contributions: SHS, DTG, and HRA: designed the study and managed the case. HKA, KAN, and AKH: contributed to the literature review, revision and table preparation. SHT: reviewed the imaging techniques used. RAY: contributed to the preparation of the manuscript. FHK and BAA: critically revised the manuscript. All authors approved the final version of the manuscript.
Use of AI: AI was not employed in drafting the manuscript, creating graphical elements, or gathering and analyzing data.
Data availability statement: The data generated by this study are fully included in the figures and/or tables of this article.
References
- Pineda-Reyes R, Cabada MM. Fascioliasis. Treatment and Management of Tropical Liver Disease 2023:83–93. doi:10.1016/B978-0-323-87031-3.00020-2.
- Salahshour F, Tajmalzai A. Imaging findings of human hepatic fascioliasis: a case report and review of the literature. Journal of Medical Case Reports 2021 15:1 2021;15(1):324. doi:10.1186/S13256-021-02945-9.
- Rinaldi L, Folliero V, Restivo L, Foglia F, Franci G, Chianese A, et al. Atypical Presentation of a Rare Parasitic Infection with Fasciola hepatica: A Multidisciplinary Case Report. Am J Case Rep 2020;21:e924704-1. doi:10.12659/AJCR.924704.
- Zali MR, Ghaziani T, Shahraz S, Hekmatdoost A, Radmehr A. Liver, spleen, pancreas and kidney involvement by human fascioliasis: imaging findings. BMC Gastroenterology 2004 4:1 2004;4(1):15-. doi:10.1186/1471-230X-4-15.
- Musa D, Godbole G, Chiodini PL, Phillips R. Unusual case of a lung abscess. Case Reports 2013;2013:bcr2012008306. doi:10.1136/BCR-2012-008306.
- Prasad S, Nassar M, Azzam AY, José FG-M-S, Jamee M, Sliman RKA, et al. CaReL Guidelines: A Consensus-Based Guideline on Case Reports and Literature Review (CaReL). Barw Medical Journal 2024;2(3):13–9. doi:10.58742/bmj.v2i2.89.
- Kakamad FH, Mohammed SH, Abdalla BA, Hussein DA, Hammood ZD, Kakamad SH, et al. Non-Recommended Publishing Lists: Strategies for Detecting Deceitful Journals. Barw Medical Journal 2026;4(1):13–21. doi:10.58742/BMJ.V4I1.227.
- Girma A, Belete Y, Afework S, Bisrat T. The Liver’s hidden foe: A case study on Human Fasciolasis. IDCases 2024;37:e02045. doi:10.1016/J.IDCR.2024.E02045.
- Liu B, Fan T, Li S. Lung Abscess. Radiology of Infectious and Inflammatory Diseases - Volume 3: Heart and Chest 2024:165–7. doi:10.1007/978-981-99-4614-3_15.
- Matin S, Joukar F, Yeganeh S, Daryakar A, Mansour-Ghanaei F. Liver Abscess due to Fasciola hepatica: A Case Report of the North of Iran. Case Rep Infect Dis 2022;2022(1):4399061. doi:10.1155/2022/4399061.
- Pınarlık F, Keske Ş, Rozanes İ, Ergönül Ö. Challenges in Diagnosis and Treatment of Fasciola hepatica Infection. Infectious Diseases & Clinical Microbiology 2023;5(1):49. doi:10.36519/idcm.2023.197.
- Castillo Almeida NE, Gurram P, Kolluri N, Pritt B, Enzler M, Suh GA. The brief case: What a fluke! A case of fascioliasis with pulmonary involvement in a peace corps volunteer. J Clin Microbiol 2020;58(10):177–97. doi:10.1128/jcm.00177-20.
- Sperling S, Dahl VN, Fløe A. Lung abscess: an update on the current knowledge and call for future investigations. Curr Opin Pulm Med 2024;30(3):229–34. doi:10.1097/MCP.0000000000001058.
- Pulpeiro JR, Armesto V, Varela J, Corredoira J. Fascioliasis: findings in 15 patients. British Journal of Radiology 1991;64(765):798–801. doi:10.1259/0007-1285-64-765-798.

Copyright (c) 2026 The Author(s)

This work is licensed under a Creative Commons Attribution 4.0 International License.