Pediatric Pilonidal Sinus Disease: A Single-Center Cohort Study of Clinical and Surgical Outcomes

Abstract
Introduction: Pilonidal sinus disease is increasingly recognized in the pediatric population, yet evidence on its clinical characteristics and surgical outcomes in children and adolescents remains limited. Given this gap, this study aimed to characterize the clinical presentation and surgical outcomes of natal cleft pilonidal sinus in a large pediatric cohort.
Methods: This retrospective cohort study included patients aged ≤18 years diagnosed with natal cleft pilonidal sinus over a five-year period. Clinical and sociodemographic data were extracted from medical records. All patients underwent minimal excision under local anesthesia with healing by secondary intention.
Results: A total of 1,751 patients were included, with a median age of 17 years and a near-equal sex distribution. Family history was positive in 65.8% of cases. Abscess formation was inversely associated with time to presentation (p < 0.001), while granuloma presence was associated with longer disease duration (p < 0.001). Females demonstrated higher abscess rates than males (30.2% vs 20.9%; p < 0.001). A positive family history was associated with earlier presentation (p = 0.007). Healing was achieved in 95.1% of cases, with a recurrence rate of 20.0% at a median follow-up of 36 months.
Conclusion: In pediatric pilonidal sinus disease, abscess and granuloma formation were associated with symptom duration, higher abscess rates in females, and earlier presentation with positive family history. Minimal excision under local anesthesia with outpatient secondary-intention healing warrants prospective comparative evaluation.
Introduction
Pilonidal sinus disease (PND) is an inflammatory condition caused by the entrapment of hair and debris within the natal cleft [1]. It predominantly affects young adults, with an estimated annual incidence of 26 cases per 100,000 individuals. The condition is most commonly seen in males during their second and third decades of life, with a male-to-female ratio of approximately 3:1 [2]. In the pediatric population, nearly 1.2 per 1,000 children are affected, with a mean age of 15 years (range: 12–19 years), and the overall prevalence appears to have increased in recent decades [3]. The disease rarely manifests before puberty, a pattern attributed to hormonal influences on the pilosebaceous glands, which become active during this developmental period [4]. While the natal cleft represents the most common site of involvement, the condition has also been documented in other anatomical locations, including the umbilicus, interdigital webs, suprapubic area, nose, groin, axilla, penis, clitoris, occiput, and prepuce [5]. The accumulation of foreign bodies and fragmented hair in moist areas of the body subsequently leads to infection and sinus formation [5]. Recognized associated factors in the pediatric population include gluteal fold hair, obesity, poor personal hygiene, and prolonged sitting, a habit particularly common among school-aged children [6]. Clinically, PND typically presents with localized inflammatory features along the sinus tract, including pain, warmth, tenderness, fluctuance, erythema, and purulent discharge. The condition is associated with recurrence and often poses significant challenges to achieving complete resolution [7].
The management of pediatric PND remains a significant clinical challenge, largely due to the absence of an established gold standard surgical technique and a paucity of high-quality evidence to guide treatment decisions [8,9]. Consequently, reported recurrence rates following surgery in children and adolescents vary considerably, ranging from 0% to 42%, and remain substantial regardless of the surgical approach employed [9,10].
This study aims to characterize the clinical presentation and surgical outcomes of pediatric PND in a large single-center cohort, addressing the limited pediatric-specific evidence in this field. Only peer-reviewed literature was cited after careful verification of all references [11].
Methods
Study Design
This retrospective single-center cohort study included pediatric patients diagnosed with natal cleft pilonidal sinus disease (NCPND) from 2020 to 2025 at a private medical facility. All patients were evaluated, treated, and followed up at the same institution. Verbal informed consent for the use of anonymized clinical data and its publication was obtained from all patients and their guardians.
Eligibility Criteria and Dataset
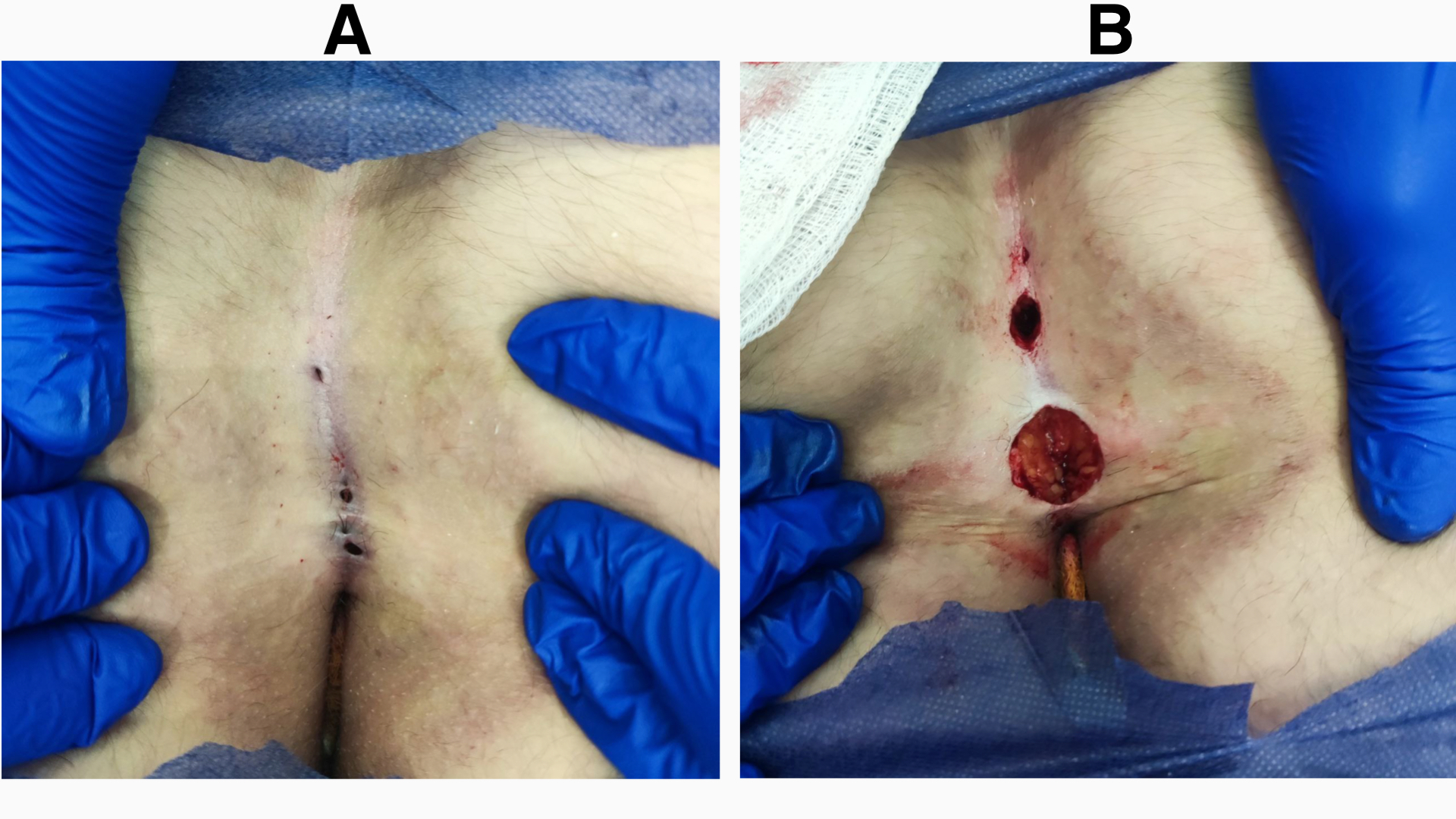
Patients aged ≤ 18 years who presented with NCPND during the study period were included. Diagnosis was established clinically based on history and physical examination, with ultrasonography being performed in cases of diagnostic uncertainty. Typical presentations included pain, swelling, discharge, itching, or midline pits in the natal cleft region (Figure 1. A). Patients managed under spinal or general anesthesia were excluded. Clinical and sociodemographic data were obtained from medical records and treating healthcare providers. Variables recorded included age, sex, presenting symptoms, past medical and surgical history, examination findings, ultrasonography findings (when performed), indications for excision under local anesthesia (LA), postoperative complications, outcome, and duration of follow-up. Time to presentation was defined as the interval between first symptom recognition and initial clinic presentation, based on patient/parent history recorded at the first encounter. As data were extracted retrospectively from existing records, individual variables were analyzed on an available-case basis, and recurrence was assessed only in the patients with a documented follow-up visit (444 [25.4%] lacked follow-up and were excluded from recurrence analysis).
Surgical Management
All procedures were performed by consultant surgeons experienced in NCPND, under the supervision of senior attending surgeons and following a standardized protocol. All patients underwent comprehensive preoperative assessment to determine suitability for LA, including monitoring of vital signs, hematological assessment, and routine viral screening, the latter performed per institutional policy for all surgical patients irrespective of anesthetic technique. All procedures were performed with the patient in the prone position using strict aseptic technique. In patients with non-acutely infected NCPND, the procedure consisted of minimal excision of the pilonidal sinus tract(s) and associated diseased tissue through a small elliptical or circular incision (specimen size approximately 1–3 cm), preserving surrounding healthy tissue, with the wound left open to heal by secondary intention (Figure 1. B). Patients presenting with acutely infected pilonidal abscesses were managed in two stages. The first stage involved incision and drainage of the abscess, followed by daily wound dressing with gauze drainage. The second stage consisted of definitive excision of the sinus tract once the acute infection had resolved. Postoperative care included analgesics as needed and daily wound dressing with normal saline until complete healing was achieved. Complete healing was defined as full epithelialization of the wound without discharge, infection, or pain and with no need for further wound care, assessed at scheduled follow-up visits with final determination at approximately 4–8 weeks. Recurrence was defined as the reappearance of pilonidal disease (sinus formation, persistent discharge, abscess, or the need for repeat intervention) at the previously treated site, diagnosed clinically during follow-up.
Statistical Analysis
The database was locked prior to analysis; data were organized using Microsoft Excel 2019 and analyzed using the Statistical Package for Social Sciences (SPSS) version 25.0. The Shapiro-Wilk and Kolmogorov-Smirnov tests were used to assess the normality of continuous variables. Continuous variables are therefore presented as median and interquartile range (IQR), while categorical variables are presented as frequencies and percentages. The chi-square test was used to assess associations between categorical variables, with Cramer's V reported as a measure of effect size. The Mann-Whitney U test was used to compare continuous variables between two independent groups. Recurrence-free survival was estimated by the Kaplan–Meier method, with time measured from the date of excision to recurrence. Patients without recurrence were censored at their last documented follow-up. Multivariable binary logistic regression was used to identify factors independently associated with abscess formation and with recurrence, with sex, time to presentation, and family history (FHX) as covariates (reference categories: <1 week and female). Results are reported as adjusted odds ratios with 95% confidence intervals, with model fit assessed by the Hosmer–Lemeshow test. Obesity was defined as BMI ≥30 kg/m², consistent with the adult threshold, which was considered appropriate given that the cohort was predominantly composed of older adolescents with a median age of 17 years. A p-value of < 0.05 was considered statistically significant.
Results
years, with a median age of 17 years (IQR = 3). Body mass index ranged from 14.1 to 43.5 kg/m², with a median of 24.4 (IQR = 5.4); by category, 884 patients (50.5%) were of normal weight, 525 (30.0%) were overweight, 221 (12.6%) were obese, and 121 (6.9%) were underweight. Overall, 881 cases were males (50.3%), and 870 were females (49.7%). Previous surgical history was positive in 124 patients (7.1%), while 1,627 (92.9%) had no history of surgical intervention. Family history for PND was positive in 1,152 cases (65.8%) and negative in 599 (34.2%). Regarding smoking status, 1,641 participants (93.7%) were non-smokers, 100 (5.7%) were active smokers, and 10 (0.6%) were passive smokers. A sedentary lifestyle was present in 1,686 participants (96.3%), while 65 (3.7%) were non-sedentary. Sitting on hard surfaces was reported in 199 patients (11.4%), and frequent car travel in 39 (2.2%), while 1,712 (97.8%) did not travel by car frequently. Body hair characteristics included a small amount in 622 cases (35.5%) and hairy in 1,129 (64.5%). Among 1,704 patients, straight hair was present in 1,409 (82.7%), wavy hair in 182 (10.7%), and curly hair in 113 (6.6%) (Table 1).
|
Age (years), median (IQR) |
17 (3) |
|
BMI (kg/m²), median (IQR) |
24.4 (5.4) |
|
BMI Classification Underweight Normal weight Overweight Obese |
121 (6.9%) 884 (50.5%) 525 (30.0%) 221 (12.6%) |
|
Sex Male Female |
881 (50.3%) 870 (49.7%) |
|
Surgical History Yes No |
124 (7.1%) 1,627 (92.9%) |
|
Family History for PND Positive Negative |
1,152 (65.8%) 599 (34.2%) |
|
Smoking Status Non-smoker Smoker Passive smoker |
1,641 (93.7%) 100 (5.7%) 10 (0.6%) |
|
Sedentary Lifestyle Yes No |
1,686 (96.3%) 65 (3.7%) |
|
Sitting on Hard Surfaces Yes No |
199 (11.4%) 1,552 (88.6%) |
|
Frequent Car Travel Yes No |
39 (2.2%) 1,712 (97.8%) |
|
Body Hair Small amount Hairy |
622 (35.5%) 1,129 (64.5%) |
|
Type of Body Hair (n=1704) Straight Wavy Curly |
1,409 (82.7%) 182 (10.7%) 113 (6.6%) |
|
IQR: interquartile range; BMI: body mass index; PND: pilonidal sinus disease |
|
Most patients were symptomatic (n = 1,729; 98.7%), with 22 (1.3%) asymptomatic; the latter were diagnosed incidentally during examination. Time to presentation was 1–12 months (n = 698; 39.9%), more than 1 year (n = 397; 22.7%), 1 week to <1 month (n = 364; 20.8%), and less than 1 week (n = 292; 16.6%). Among symptomatic patients, pain was reported in 1,573 patients (91.0%), itching in 1,080 (62.5%), discharge in 984 (57.0%), of whom 753 (43.5%) had purulent discharge, and swelling in 685 (39.6%). On examination, a sinus tract was identified in 1,726 patients (98.6%), abscess formation in 447 (25.5%; 95% CI 23.5–27.6), and granuloma in 313 (17.9%; 95% CI 16.2–19.7). As for treatment outcomes, healing was assessed at the treating center for all 1,751 patients and was achieved in 1,666 (95.1%; 95% CI 94.0–96.1), while 85 (4.9%) did not achieve complete healing. Recurrence assessment required follow-up data, which were available for 1,307 patients (74.6%); the remaining 444 (25.4%) lacked follow-up. Among the 1,307 patients with follow-up data, 262 (20.0%; 95% CI 18.0–22.3) experienced recurrence and 1,045 (80.0%) did not, over a median follow-up of 36 months (IQR = 25); of those who recurred, 246 (94.0%) did so after documented initial healing, while 16 (6.0%) represented persistent disease in patients who had not achieved initial healing (Table 2).
|
Variable |
Frequency/percentages |
|
Symptom Status Symptomatic Asymptomatic |
1,729 (98.7%) 22 (1.3%) |
|
Time to Presentation After PND 1–12 months More than 1 year 1 week–<1 month Less than one week |
698 (39.9%) 397 (22.7%) 364 (20.8%) 292 (16.6%) |
|
Symptoms (n=1729) Pain Itching Discharge Swelling |
1,573 (91.0%) 1,080 (62.5%) 984 (57.0%) 685 (39.6%) |
|
Examination Findings Sinus tract Abscess formation Granuloma |
1,726 (98.6%) 447 (25.5%) 313 (17.9%) |
|
Number of Sinus Openings 1 2 3 4 5 6 ≥7 |
377 (21.5%) 402 (23.0%) 335 (19.1%) 236 (13.5%) 134 (7.7%) 98 (5.6%) 169 (9.6%) |
|
Healing Status Achieved Not achieved |
1,666 (95.1%) 85 (4.9%) |
|
Recurrence (n = 1,307) Present Absent |
262 (20.0%) 1,045 (80.0%) |
|
Recurrence by healing status (n = 262) After initial healing Persistent disease (no initial healing) |
246 (94.0%) 16 (6.0%) |
|
PND: pilonidal sinus disease |
|
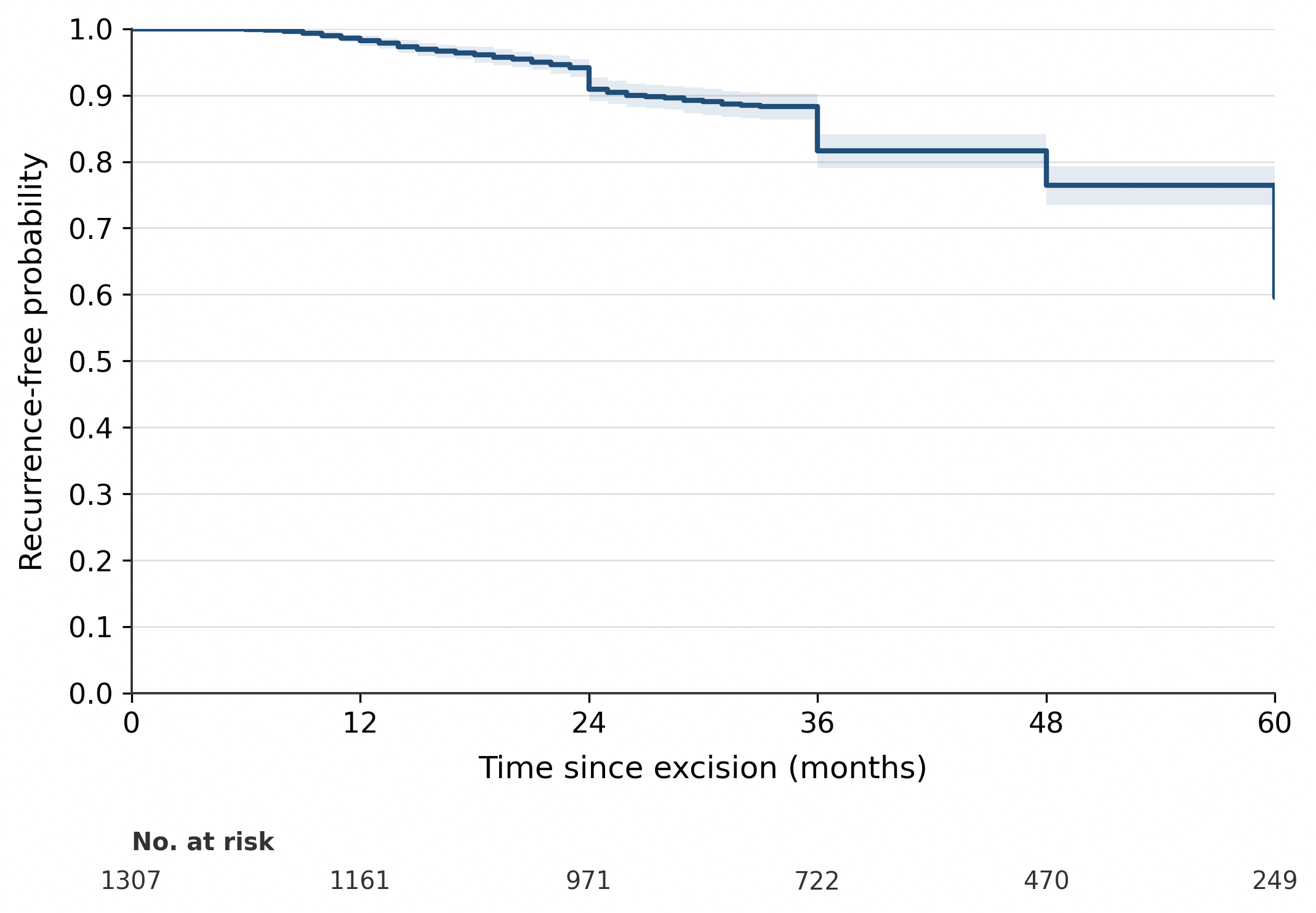
A significant association was found between granuloma presence and time to presentation (χ² = 77.198, df = 3, p < 0.001; Cramer's V = 0.21), with granuloma present in 4.8% of patients presenting within one week, 11.3% within 1 week to <1 month, 21.1% within 1–12 months, and 28.0% after more than one year. Abscess formation was similarly associated with time to presentation (χ² = 431.851, df = 3, p < 0.001; Cramer's V = 0.50), present in 67.1% of patients within one week, 38.2% within 1 week to <1 month, 9.5% within 1–12 months, and 11.6% after more than one year (Table 3). Furthermore, females demonstrated a higher rate of abscess formation compared to males (30.2% vs 20.9%; χ² = 20.105, df = 1, p < 0.001; Cramer's V = 0.11). However, FHX was not significantly associated with recurrence (20.8% vs 18.6%; χ² = 0.867, p = 0.352; Cramer's V = 0.03), nor was obesity (18.6% vs 20.3%; χ² = 0.257, p = 0.612; Cramer's V = 0.014) (Table 4). Patients with a positive FHX of NCPND presented at a younger age than those without FHX (median 16 vs 17 years; U = 318,462, p = 0.007) (Table 5). Kaplan–Meier recurrence-free probability declined from 90.9% at 24 months to 59.6% at 60 months (Figure 2).
|
Variable |
< 1 week |
1 week–<1 month |
1–12 months |
> 1 year |
χ² |
p-value |
Cramer's V | |
|
Granuloma
|
Absent |
278 (95.2%) |
323 (88.7%) |
551 (78.9%) |
286 (72.0%) |
77.198 |
<0.001 |
0.21 |
|
Present |
14 (4.8%) |
41 (11.3%) |
147 (21.1%) |
111 (28.0%) |
||||
|
Abscess
|
Absent |
96 (32.9%) |
225 (61.8%) |
632 (90.5%) |
351 (88.4%) |
431.851 |
<0.001 |
0.50 |
|
Present |
196 (67.1%) |
139 (38.2%) |
66 (9.5%) |
46 (11.6%) |
||||
| χ²: Chi-Square statistic | ||||||||
|
Variable |
Category |
Status n (%) |
χ² |
p-value |
Cramer's V |
|
|
Yes |
No |
|||||
|
Abscess formation by sex |
Male |
184 (20.9%) |
697 (79.1%) |
20.105 |
<0.001 |
0.11 |
|
Female |
263 (30.2%) |
607 (69.8%) |
||||
|
FHX by Rx |
Positive FHX |
178 (20.8%) |
678 (79.2%) |
0.867 |
0.352 |
0.03 |
|
Negative FHX |
84 (18.6%) |
367 (81.4%) |
||||
|
Obesity by Rx |
Obese |
32 (18.6%) |
140 (81.4%) |
0.257
|
0.612
|
0.014
|
|
Not Obese |
230 (20.3%) |
905 (79.7%) |
||||
|
Comparison |
Category |
Age, median (IQR), years |
U |
p |
|
Age at Presentation
|
Positive FHX |
16 (2) |
318,462
|
0.007
|
|
Negative FHX |
17 (3) |
|||
|
IQR: interquartile range; U: Mann-Whitney U test; FHX: family history |
||||
In multivariable logistic regression for abscess formation, earlier presentation and female sex were independently associated with higher odds of abscess. Relative to presentation within one week, the adjusted odds of abscess were markedly lower at 1 week to <1 month (OR 0.30, 95% CI 0.22–0.42), 1–12 months (OR 0.05, 95% CI 0.04–0.07), and beyond one year (OR 0.07, 95% CI 0.04–0.10; all p < 0.001). Male sex was associated with lower odds of abscess relative to female sex (OR 0.63, 95% CI 0.49–0.81, p < 0.001), whereas FHX was not independently associated with abscess (OR 1.20, 95% CI 0.92–1.56, p = 0.177). The model showed good fit (Hosmer-Lemeshow p = 0.42; Nagelkerke R² = 0.32) (Table 6). In the model for recurrence, restricted to the 1,307 patients with available follow-up data (262 events), none of the examined factors was independently associated with the outcome. Neither time to presentation (overall p = 0.72), sex (OR 1.15, 95% CI 0.87–1.51, p = 0.320), nor FHX (OR 1.17, 95% CI 0.87–1.57, p = 0.293) predicted recurrence, and the model was not statistically significant overall (Omnibus p = 0.68), explaining negligible variance (Nagelkerke R² < 0.01). Model calibration was nonetheless adequate (Hosmer–Lemeshow p = 0.98). These findings indicate that recurrence was not predicted by the baseline clinical characteristics examined (Table 7).
|
Variable |
Adjusted OR |
95% CI |
p-value |
|
Sex (male vs female) |
0.63 |
0.49–0.81 |
<0.001 |
|
Time to presentation (ref: <1 week) |
|||
|
1 week–<1 month |
0.30 |
0.22–0.42 |
<0.001 |
|
1–12 months |
0.05 |
0.04–0.07 |
<0.001 |
|
>1 year |
0.07 |
0.04–0.10 |
<0.001 |
|
Family history (positive vs negative) |
1.20 |
0.92–1.56 |
0.177 |
| OR: odds ratio; CI: confidence interval. Reference categories: female sex and presentation within one week. Model fit: Hosmer–Lemeshow p = 0.42; Nagelkerke R2 = 0.32. | |||
|
Variable |
Adjusted OR |
95% CI |
p-value |
|
Time to presentation (ref: <1 week) |
|||
|
1 week–<1 month |
0.78 |
0.51–1.22 |
0.276 |
|
1–12 months |
0.88 |
0.60–1.29 |
0.499 |
|
>1 year |
0.82 |
0.54–1.26 |
0.363 |
|
Sex (male vs female) |
1.15 |
0.87–1.51 |
0.320 |
|
Family history (positive vs negative) |
1.17 |
0.87–1.57 |
0.293 |
|
OR: odds ratio; CI: confidence interval. Reference categories: female sex and presentation within one week. Overall model not significant (omnibus p = 0.68); Hosmer–Lemeshow p = 0.98; Nagelkerke R2 < 0.01. |
|||
Discussion
This large single-center cohort of 1,751 pediatric patients characterized the clinical associations and surgical outcomes of NCPND managed by minimal excision under local anesthesia. The principal findings were that abscess formation was strongly associated with earlier presentation and female sex, granuloma with longer symptom duration, and positive FHX with younger age at presentation, while no baseline factor independently predicted recurrence. Complete healing was achieved in 95.1% of patients, with a crude recurrence rate of 20.0%. Surgical options in treating PND include excision with primary closure, secondary intention healing, off-midline flap procedures, and minimally invasive techniques, each with distinct trade-offs between healing time and complication rates [9,12]. More recently, minimally invasive approaches have gained popularity due to minimal postoperative pain and earlier return to normal activities, as well as significantly shorter operative times [1,8].
In this study, a near-equal male-to-female ratio was observed (50.3% male vs. 49.7% female), contrasting with the 3:1 to 4:1 male predominance ratio reported in adults [13]. However, this finding is consistent with other pediatric series, including the 1:1.14 ratio reported by Ozcan et al., as well as distributions reported by Nasr and Ein (52.9% male) and Esposito et al. (55.6% male) [8,13,14]. Nevertheless, female predominance has also been described by other studies, such as Lee et al. (55.6% and 82.2% female across treatment groups) and Kalyoncu Ayçenk (62.0% female) [1,6]. Collectively, these discrepancies suggest that the traditional male predominance may be less pronounced in pediatric populations, particularly in younger age groups.
Family history emerged as a notably prominent finding in the present study, with FHX documented in 65.8% of patients, a proportion considerably higher than that reported in comparable studies of adolescent and young adult populations. Yildiz et al. identified a positive FHX in 52.4% of their teenage cohort, while Kalyoncu Ayçenk reported this in 32.0% of patients, and the meta-analysis by Xu et al. yielded a pooled prevalence of 29.6% across included studies [6,15,16]. Notably, FHX was self-reported by patients and guardians, based on FHX in any relative, and not independently verified. This method is prone to recall bias and may over-report prevalence, likely contributing to the higher rate observed here. The clinical significance of hereditary predisposition has been well demonstrated by Yildiz et al., who found that familial transmission was significantly more prevalent in patients with NCPND compared to healthy controls (OR: 8.652, p = 0.005) [15]. This elevated prevalence may reflect a more pronounced genetic predisposition within the studied population, or regional or ethnic variation in heritability. In the study herein, patients with a positive FHX of NCPND presented at a significantly younger age (median 16 vs 17 years; U = 318,462, p = 0.007), although this one-year difference, while statistically significant, is likely of limited clinical relevance. A similar trend was reported by Doll et al. in an adult cohort, where patients with a positive FHX underwent surgery at a younger age compared to those without FHX (22.4 vs 23.9 years, p = 0.038), supporting the concept of earlier disease manifestation in genetically predisposed individuals [17]. Although the Doll et al. study was conducted in adults, the consistency of this finding in the present pediatric cohort suggests that FHX exerts a similar influence on disease onset across age groups. In contrast, FHX was not significantly associated with recurrence (20.8% vs 18.6%; χ² = 0.867, p = 0.352), which differs from the long-term recurrence trends reported by Doll et al., likely attributable to the considerably shorter follow-up period in the present study [17].
A sedentary lifestyle was recorded in 96.3% of patients; however, this was based on patient self-report and parental report rather than a standardized cutoff such as the ≥6 hours/day threshold used by Yildiz et al., who reported prolonged sitting in 45.2% of their cohort. The absence of a quantitative definition likely explains the higher proportion observed here [15]. Regarding body hair characteristics, 64.5% of patients were observed to be hairy, though formal assessment of hirsutism was not performed. This is consistent with the broader literature, in which dense body hair is recognized as a significant risk factor for NCPND (OR: 3.29), and hirsutism has been identified as a predisposing factor in multiple studies [2,8,16]. Notably, straight hair was the most common hair type in this cohort (82.7%), in contrast to curly hair, which Xu et al. identified as a risk factor [16]. However, this likely reflects the underlying hair-type distribution of the regional population rather than a true contradiction.
Granuloma presence was associated with longer disease duration (χ² = 77.198, p < 0.001; Cramer's V = 0.21), being identified in 4.8% of patients presenting within one week compared to 28.0% of those presenting after more than one year. This supports the interpretation of granuloma as a marker of chronic disease. According to the established pathogenesis, granuloma formation develops gradually as a foreign body reaction to hair penetration into the subcutaneous tissue, leading to progressive inflammation and tract epithelialization over time, which explains why granulomas are more frequently identified in long-standing disease [18]. In contrast, a strong inverse association was observed between time to presentation and abscess formation (χ² = 431.851, p < 0.001; Cramer's V = 0.50), with abscess markedly less common with later presentation, occurring in 67.1% of patients presenting within one week compared with 11.6% of those presenting after more than one year. This relationship persisted on multivariable analysis, with progressively lower odds of abscess at each later interval (OR 0.30 at 1 week to <1 month, 0.05 at 1–12 months, and 0.07 beyond one year, relative to presentation within one week; Nagelkerke R² = 0.32), indicating it was not attributable to the other characteristics examined. This pattern reflects the acute nature of abscess formation, which arises from rapid bacterial proliferation within an obstructed sinus pit, resulting in pain, swelling, and a purulent collection that prompts early presentation [18,19]. Although these mechanisms have been primarily described in adult populations, the present findings indicate that the same disease behavior is observable in pediatric patients, reinforcing the relevance of these pathogenic principles across age groups.
Among the present cohort, females demonstrated higher abscess rates than males (30.2% vs 20.9%; χ² = 20.105, p < 0.001; Cramer's V = 0.11). Directly comparable pediatric abscess-prevalence data by sex are scarce; the closest available comparison, Stoeckel et al., reported a higher frequency of incision and drainage in females (6.0% vs 3.0%, p = 0.01), though as a procedural rather than a prevalence metric, so the two are not directly comparable [20]. Chiu et al. similarly observed sex-related differences in pain intensity, drainage, and granuloma formation among pediatric patients, proposing hormonal influences during puberty as a potential underlying mechanism [21]. Taken together, these findings suggest that the higher abscess rate observed among females in this cohort reflects a sex-specific clinical pattern in adolescents rather than greater disease burden.
In the present study, healing by secondary intention following minimal excision under LA was achieved in 95.1% of patients. The published literature consistently reports longer healing times with secondary intention compared to primary closure, though primary closure carries its own morbidity, most notably wound dehiscence [9]. Additionally, primary closure was performed as an inpatient procedure, with a median hospital stay of up to 15.8 days reported in one case series [3]. The outpatient approach employed here avoided inpatient admission, although the two-stage management of abscesses entailed repeat outpatient visits. While this may represent a clinically meaningful advantage in patient burden and resource use, in the absence of a comparator arm it is inferred rather than demonstrated and would require prospective comparative evaluation to confirm.
Recurrence remains the principal challenge in pediatric NCPND. The crude rate of 20.0% at a median follow-up of 36 months is consistent with the 26.0% pooled risk for excision with open healing reported by Hardy et al. [9] and with comparable series [13,14]. This crude figure, however, reflects events observed during available follow-up: Kaplan–Meier analysis showed recurrence-free probability falling from 90.9% at 24 months to 59.6% at 60 months, corresponding to a cumulative recurrence of 40.4% as later recurrences accrued beyond the second postoperative year. This trajectory closely mirrors the largest longitudinal pediatric datasets, in which five-year recurrence reaches approximately 46.0% and is roughly fourfold higher than in adults [10], indicating that the high long-term recurrence reflects an age-related disease pattern rather than a shortcoming of the technique, and underscoring the need for prospective evaluation with sustained follow-up. Obesity was not associated with recurrence in this cohort (18.6% vs 20.3%; p = 0.612), consistent with most pediatric data. Esposito et al. found no association on multivariable analysis (OR 0.934, p = 0.795), and Ozcan et al. reported no significant BMI difference between patients with and without recurrence (p = 0.167) [13,22]. This suggests that obesity, although implicated in the development of pilonidal disease, may not influence recurrence once disease is established.
This study has several limitations inherent to its retrospective, single-center design, including the potential for selection bias and limited generalizability. As data were drawn from a single private facility, the cohort may be subject to referral and socioeconomic bias and may not reflect the broader pediatric population. The exclusion of patients managed under spinal or general anesthesia may also have introduced selection bias, as the cohort was limited to those suitable for local anesthesia and may not represent patients with more extensive or complex disease. The absence of a control group precluded formal comparative risk factor analysis, and several recognized risk factors, including obesity, sedentary lifestyle, and hirsutism, were recorded descriptively rather than systematically measured, limiting their interpretation. Key exposure variables, including FHX and time to presentation, were self-reported and unverified, introducing potential recall bias. Additionally, the large sample size may have inflated statistical significance for some findings, and clinical interpretability should be considered accordingly. Furthermore, incomplete follow-up data for a subset of patients may introduce attrition bias and limit the accuracy of recurrence estimates. Recurrence may also be underestimated, as follow-up relied on documented clinical encounters rather than active surveillance.
Conclusion
In conclusion, abscess and granuloma formation in pediatric NCPND were associated with symptom duration, higher abscess rates in females, and earlier presentation with positive FHX. Minimal excision under local anesthesia with outpatient secondary-intention healing warrants prospective comparative evaluation.
Declarations
Conflicts of interest: The authors declare no conflicts of interest.
Ethical approval: As the study design was a retrospective cohort study based on the analysis of existing clinical records, formal ethical approval was not required in accordance with institutional policy.
Consent for participation: Not applicable.
Consent for publication: Verbal informed consent for publication of anonymized data was obtained from all patients and their legal guardians.
Funding: No funding was received for conducting this study.
Acknowledgements: None.
Authors' contributions: AMS: involved in study conceptualization, design, and methodology, the management and surgery of all cases, and critical review and follow-up of cases. ISS and MSJ: involved in study conceptualization, design, and methodology, as well as critical review of the manuscript. MTH: involved in methodology, writing the first draft of the manuscript, data curation and analysis, and visualization. OAA, HAHM, KQA, and THH: involved in data curation and critical review of the manuscript. AAQ, BLF, AOH, and KZH: involved in critical review of the manuscript and follow-up of patients. HOA: involved in critically reviewing the manuscript. All authors read and approved the final version of the manuscript.
Use of AI: The authors used Claude Opus 4.7 and Claude Opus 4.8 (Anthropic, PBC, San Francisco, CA, USA) to check the language and flow of the manuscript; the authors have reviewed the manuscript and take full responsibility for its content.
Data availability statement: The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
- Lee WG, Short C, Zhong A, Vojvodic V, Sundin A, Spurrier RG, et al. Outcomes of pediatric pilonidal disease treatment: excision with off-midline flap reconstruction versus endoscopic pilonidal sinus treatment. Pediatric Surgery International. 2024;40(1):46. doi:10.1007/s00383-023-05629-1
- Tam A, Steen CJ, Chua J, Yap RJ. Pilonidal sinus: an overview of historical and current management modalities. Updates in Surgery. 2024;76(3):803-10. doi:10.1007/s13304-024-01799-2
- Pfammatter M, Erlanger TE, Mayr J. Primary transverse closure compared to open wound treatment for primary pilonidal sinus disease in children. Children. 2020;7(10):187. doi:10.3390/children7100187
- Arda İS, Güney LH, Sevmiş Ş, Hiçsönmez A. High body mass index as a possible risk factor for pilonidal sinus disease in adolescents. World journal of surgery. 2005;29(4):469-71. doi:10.1007/s00268-004-7533-y
- Faraj FH, Baba HO, Salih AM. Risk factors of pilonidal sinus disease in preparatory school students; a case control study. Annals of Medicine and Surgery. 2020;57:46-8. doi:10.1016/j.amsu.2020.07.016
- Ayçenk AK. Use of crystallized phenol in pilonidal sinus, in the pediatric age group, 5-year single surgeon experience. Interdisciplinary Medical Journal. 2024;15(53):118-22. doi:10.17944/interdiscip.1475704
- Salih AM, Kakamad FH, Salih RQ, Mohammed SH, Habibullah IJ, Hammood ZD, et al. Nonoperative management of pilonidal sinus disease: one more step toward the ideal management therapy—a randomized controlled trial. Surgery. 2018;164(1):66-70. doi:10.1016/j.surg.2017.12.014
- Esposito C, Mendoza-Sagaon M, Del Conte F, Cerulo M, Coppola V, Esposito G, et al. Pediatric endoscopic pilonidal sinus treatment (PEPSiT) in children with pilonidal sinus disease: tips and tricks and new structurated protocol. Frontiers in Pediatrics. 2020;8:345. doi:10.3389/fped.2020.00345
- Hardy EJ, Herrod PJ, Doleman B, Phillips HG, Ranat R, Lund JN. Surgical interventions for the treatment of sacrococcygeal pilonidal sinus disease in children: a systematic review and meta-analysis. Journal of pediatric surgery. 2019;54(11):2222-33. doi:10.1016/j.jpedsurg.2019.02.058
- Doll D, Haas S, Faurschou IK, Hackmann T, Heitmann H, Braun-Münker M, et al. Pediatric pilonidal sinus disease: recurrence rates of different age groups compared to adults. Surgery Open Science. 2025;23:50-6. doi:10.1016/j.sopen.2025.01.001
- Kakamad FH, Mohammed SH, Abdalla BA, Hussein DA, Hammood ZD, Kakamad SH, et al. Non-Recommended Publishing Lists: Strategies for Detecting Deceitful Journals. Barw Med J. 2026;4(1):13–21. doi:10.58742/bmj.v4i1.227
- Salih AM, Ahmed MM, Baba HO, Kakamad FH, Salih KM, Muhedin SS, et al. Non‐operative management of pilonidal sinus disease; classification and outcome. International Wound Journal. 2023;20(9):3639-47. doi:10.1111/iwj.14242
- Ozcan R, Hüseynov M, Bakır AC, Emre S, Tütüncü C, Celayir S, et al. Which treatment modality for pediatric pilonidal sinus: Primary repair or secondary healing?. Asian journal of surgery. 2018;41(5):506-10. doi:10.1016/j.asjsur.2017.08.006
- Nasr A, Ein SH. A pediatric surgeon’s 35-year experience with pilonidal disease in a Canadian children’s hospital. Canadian Journal of Surgery. 2011;54(1):39. doi:10.1503/cjs.028509
- Yildiz T, Elmas B, Yucak A, Turgut HT, Ilce Z. Risk factors for pilonidal sinus disease in teenagers. The Indian Journal of Pediatrics. 2017;84(2):134-8. doi:10.1007/s12098-016-2180-5
- Xu X, You P, Qin J, Wu J. Risk factors for sacrococcygeal pilonidal sinus: a systematic review and meta-analysis supplemented by genetic causal assessment. Frontiers in Surgery. 2025;12:1718589. doi:10.3389/fsurg.2025.1718589
- Doll D, Matevossian E, Wietelmann K, Evers T, Kriner M, Petersen S. Family history of pilonidal sinus predisposes to earlier onset of disease and a 50% long-term recurrence rate. Diseases of the colon & rectum. 2009;52(9):1610-5. doi:10.1007/DCR.0b013e3181a87607
- Khanna A, Rombeau JL. Pilonidal disease. Clinics in colon and rectal surgery. 2011;24(01):046-53. doi:10.1055/s-0031-1272823
- Karatas T, Kanlioz M. The correlation between delayed surgical therapy after the diagnosis of pilonidal sinus disease and relapse, labor loss, and costs. Cureus. 2019;11(11):1-5. doi:10.7759/cureus.6255
- Stoeckel A, Murtadi G, Renzi K, McArthur M, Cohen R, Mooney DP. Gender differences in adolescent pilonidal disease. Journal of pediatric surgery. 2025;60(5):162267. doi:10.1016/j.jpedsurg.2025.162267
- Chiu B, Abrajano C, Shimada H, Yousefi R, Dalusag K, Adams M, Su W, Hui T, Mueller C, Fuchs J, Dunn J. Differences between male and female patients with pilonidal disease. Journal of Pediatric Surgery Open. 2024;6:100132. doi:10.1016/j.yjpso.2024.100132
- Esposito C, Leva E, Gamba P, Sgrò A, Ferrentino U, Papparella A, et al. Pediatric endoscopic pilonidal sinus treatment (PEPSiT): report of a multicentric national study on 294 patients. Updates in Surgery. 2023;75(6):1625-31. doi:10.1007/s13304-023-01508-5

Copyright (c) 2026 The Author(s)

This work is licensed under a Creative Commons Attribution 4.0 International License.