Multifocal Fibrosing Thyroiditis: A High-Volume Center Experience

Abstract
Introduction: Multifocal fibrosing thyroiditis (MFT) is a rare and underrecognized fibroinflammatory lesion of the thyroid characterized by multiple discrete fibrotic foci with reactive epithelial changes. Its morphologic overlap with papillary thyroid carcinoma (PTC) and its reported coexistence with PTC have generated ongoing debate regarding its clinical and biological significance. The primary aim of this study is to characterize the clinicopathologic features of MFT across a large single-center experience.
Methods: A retrospective case series was conducted at a single endocrine center between October 2022 and January 2026. All patients with histopathologically confirmed MFT were included. Demographic, clinical, laboratory, radiologic, surgical, and histopathologic data were collected and analyzed descriptively.
Results: Twenty-seven patients were identified, with a mean age of 45.1 ± 8 years, of whom 22 (81.5%) were female. Twenty-four patients underwent total thyroidectomy (88.9%). Concurrent PTC was identified in 11 cases (40.7%). Among the 11 PTC cases, 8 (72.7%) were unifocal, and 3 (27.3%) were multifocal.
Conclusion: Multifocal fibrosing thyroiditis is a rare thyroid lesion with distinctive histopathologic features. Greater awareness of this entity may improve diagnostic accuracy and clarify its clinical significance.
Introduction
Multifocal fibrosing thyroiditis (MFT) is a rare and underrecognized fibroinflammatory lesion of the thyroid gland characterized by multiple discrete fibrotic foci composed of a paucicellular central fibrotic core surrounded by a more cellular peripheral zone containing reactive-appearing follicular epithelial atypia and variable chronic inflammatory infiltrates [1].
Since its original description in 1990 [2], the etiology and pathogenesis of MFT have remained speculative. Various hypotheses have been proposed, including localized parenchymal injury, stromal remodeling, and a reactive process occurring in the setting of other thyroid pathology; however, no definitive mechanism has been established [1,3]. Frequently, MFT is discovered incidentally during histopathologic examination of thyroidectomy specimens resected for suspicious nodules, multinodular goiter, or coexisting thyroid malignancy rather than as a primary clinical diagnosis [1].
Recently, it has been suggested that MFT is analogous to a radial scar lesion in breast tissue both in morphology and pathogenesis, as the fibrotic lesion is a risk factor for the development of carcinoma [4-6]. Radial scars are often found incidentally on breast biopsies or mastectomies performed for other indications [5]. Multifocal fibrosing thyroiditis, like radial scars, shows a stellate configuration with fibro-elastotic center entrapping epithelial structures, and proliferative regenerative change in the surrounding parenchyma [4].
Although the clinicopathological significance of MFT remains incompletely defined, MFT has increasingly been reported in association with papillary thyroid carcinoma (PTC), raising questions regarding its potential role as a reactive or premalignant process [1,3].
This study aims to present a case series of MFT and to provide a brief review of the existing literature. The references were assessed for credibility using the most current evaluation criteria [7].
Methods
Study Design and Setting
This retrospective case series included patients managed between October 2022 and January 2026. The hospital is a regional referral center for endocrine surgery, assessing 75,000 patients with thyroid disorders over the 3-year study period.
Inclusion and Exclusion Criteria
Inclusion criteria comprised all patients with a histopathologically confirmed diagnosis of MFT [8] following surgical intervention. Patients with incomplete medical records, insufficient follow-up data, or lacking definitive histopathological confirmation were excluded from the study.
Data Collection
Data were extracted from the hospital's electronic medical records and pathology databases. The collected variables included demographic information, clinical presentation, medical history, details of surgical procedures, histopathological findings, and tumor characteristics (size, presence of extra-thyroidal extension, lymphatic-vascular invasion). Preoperative imaging, such as high-resolution neck ultrasonography, was reviewed to assess tumor localization and extent. Biochemical parameters, including thyroid function tests and serum thyroglobulin, were recorded preoperatively and during follow-up.
Histopathological Analysis
For histopathological analysis, 5‑μm‑thick tissue sections were fixed in 10% neutral buffered formalin at room temperature for 1–3 days, routinely processed, paraffin-embedded, and sectioned. Sections were stained with hematoxylin and eosin using an automated staining system.
Surgical Intervention
All patients underwent surgical intervention under general anesthesia, performed by experienced endocrine surgeons. The choice of surgical procedure, ranging from total thyroidectomy, thyroid lobectomy, or partial lobectomy, was determined based on preoperative imaging, intraoperative findings, and clinical judgment. Efforts were made to preserve critical anatomical structures, including the recurrent laryngeal nerve and adjacent vascular structures. In cases with suspected malignancy or invasive characteristics, wider excision margins were pursued to minimize residual disease. Lymph node dissection was performed when there was clinical or radiological suspicion of nodal involvement.
Data Analysis
Collected data were entered into Microsoft Excel 2021 and subsequently analyzed using the Statistical Package for the Social Sciences (SPSS) software, version 27.0. Descriptive statistics were employed to summarize the data, with continuous variables presented as mean ± standard deviation. Categorical variables were expressed as frequencies and percentages. Normality of continuous variables (age, thyroid stimulating hormone [TSH], free thyroxine [free T4]) was assessed using the Shapiro-Wilk test and showed normal distribution. Accordingly, continuous variables are presented as mean ± standard deviation (SD).
Results
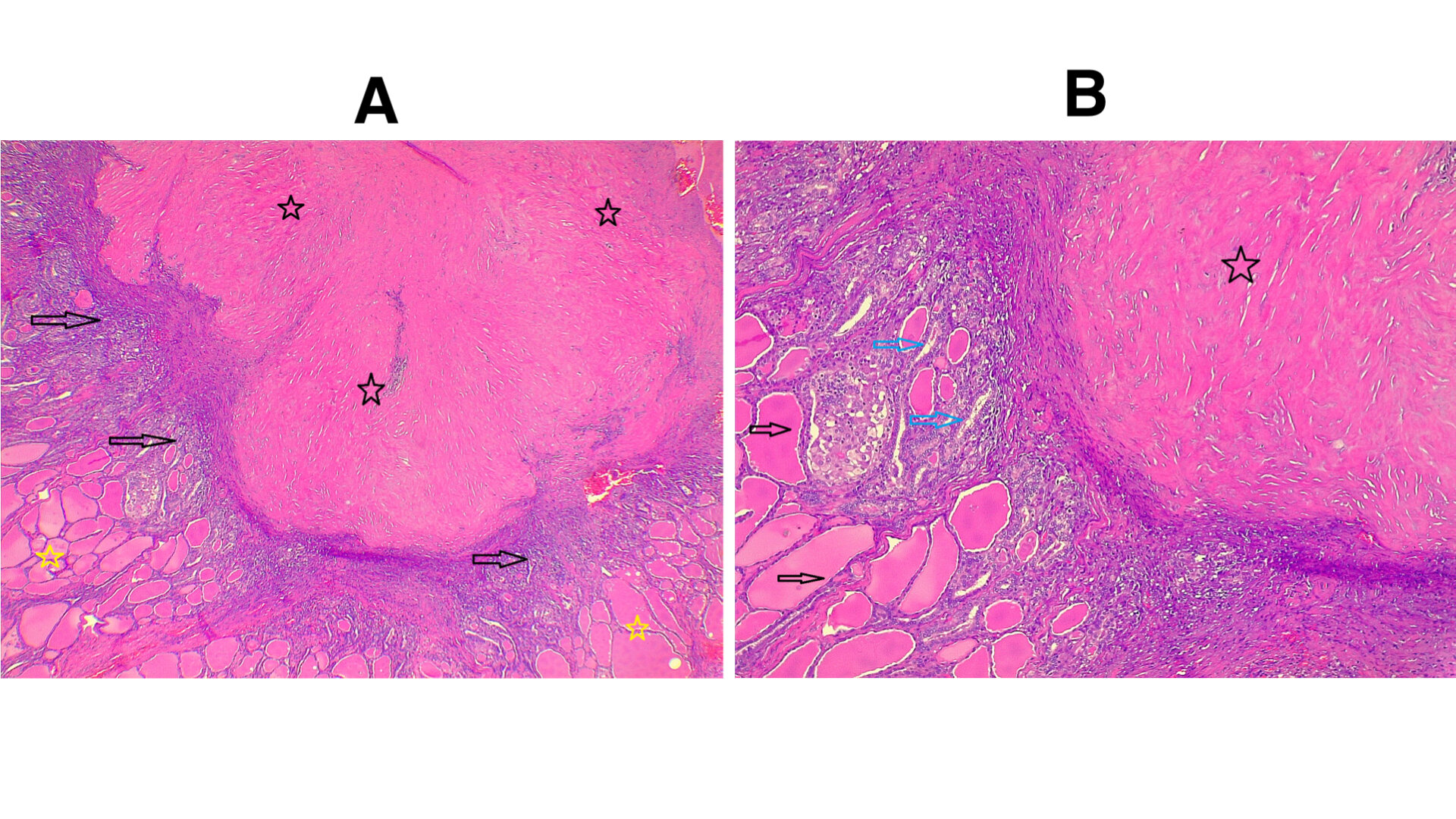
This study included 27 patients with histologically confirmed MFT (Figure 1) (composing 0.04% of all thyroid disorders). The mean age was 45.1 ± 8 years, with a range of 26 to 68 years, comprising 22 female patients (81.5%) and 5 male patients (18.5%). The most frequent clinical presentation was generalized weakness, observed in 7 patients (25.9%). Eighteen patients (66.7%) reported no significant past medical history. Regarding past surgical history, 19 patients (70.4%) had undergone previous surgical procedures, while 8 patients (29.6%) had no history of prior surgery. The most frequently reported prior operation was caesarean section, documented in 13 patients (48.1%), with 6 patients undergoing other surgeries (Table 1).
|
Variables |
Frequency |
|
Sex Female Male |
22 (81.5%) 5 (18.5%) |
|
Age groups (years) 26-36 37-47 48-58 59-69 Mean ± SD |
2 (7.4%) 16 (59.3%) 8 (29.6%) 1 (3.7%) 45.1 ± 8 years |
|
Smoking status Active smoker Passive smoker Non-smoker |
3 (11.1%) 4 (14.8%) 20 (74.1%) |
|
Family history Positive for PTC Negative |
3 (11.1%) 24 (88.9%) |
|
Past medical history Negative Hypertension only HTN + CKD DM + HTN HTN + GIST PCOS TB |
18 (66.7%) 3 (11.1%) 2 (7.4%) 1 (3.7%) 1 (3.7%) 1 (3.7%) 1 (3.7%) |
|
Past surgical history C/S Other Negative |
13 (48.1%) 6 (22.2%) 8 (29.6%) |
|
Clinical presentation Generalized weakness Weight loss Palpitation Anterior neck swelling Lateral neck swelling Globus sensation Voice change Incidental |
7 (25.9%) 5 (18.5%) 4 (14.8%) 2 (7.4%) 3 (11.1%) 2 (7.4%) 1 (3.7%) 3 (11.1%) |
|
SD: standard deviation; PTC: papillary thyroid carcinoma; HTN: hypertension; DM: diabetes mellitus; GIST: gastro intestinal stromal tumor; PCOS: polycystic ovarian syndrome; CKD: chronic kidney disease; TB: tuberculosis; PSH: past surgical history; C/S: caesarean section |
|
Preoperative thyroid function test was conducted, with a mean TSH of 2.07 ± 1.4, ranging from 0.005 to 5.14 uIU/ml, and serum free T4 of 16.45 ± 2.5, ranging from 12.3 to 22 pmol/L. Neck ultrasound examinations were conducted for 25 patients (92.6%). In 24 patients (88.9%), at least one nodule was recorded with Thyroid Imaging Reporting and Data System (TI-RADS) classifications ranging from TR3 to TR5. Five patients (18.5%) had TR3 nodules, while TR4 nodules were identified in 16 patients (59.3%). TR5 nodules were observed in 3 patients (11.1%). Fine needle aspiration cytology (FNAC), conducted on 17 patients (62.9%), demonstrated varying probabilities of malignancy, ranging from Bethesda I to Bethesda VI. Surgical management primarily involved total thyroidectomy, which was performed in 24 patients (88.9%). Thyroid lobectomy, with or without parathyroidectomy, was undertaken in 3 patients (11.1%), including 2 procedures on the right lobe (7.4%) and 1 on the left lobe (3.7%). In 11 patients (40.7%), concurrent thyroid carcinoma was present, all of which were papillary type PTC (100%) (Table 2).
|
Variables |
Frequency |
|
TSH (uIU/ml) <0.4 0.4-4 4.1-10 Mean ± SD |
4 (14.8%) 20 (74.1%) 3 (11.1%) 2.07 ± 1.4 |
|
Free T4 (pmol/L) 12-22 Mean ± SD |
27 (100.0%) 16.45 ± 2.51 |
|
Ultrasound One nodule MNG Thyroiditis with nodule Findings suggestive of GD Not done |
2 (7.4%) 21 (77.8%) 1 (3.7%) 1 (3.7%) 2 (7.4%) |
|
TI-RADS TR-1 TR-2 TR-3 TR-4 TR-5 Not available |
0 (0.00%) 0 (0.00%) 5 (18.5%) 16 (59.3%) 3 (11.1%) 3 (11.1%) |
|
FNA Bethesda classification B I B II B III B IV B V B VI Not done |
3 (11.1%) 5 (18.5%) 2 (7.4%) 0 (0.00%) 1 (3.7%) 6 (22.2%) 10 (37.0%) |
|
Procedure Total Thyroidectomy Right lobectomy + Right CLND Right partial lobectomy Left lobectomy |
24 (88.9%) 1 (3.7%) 1 (3.7%) 1 (3.7%) |
|
Histological Diagnosis MFT PTC and MFT |
16 (59.3%) 11 (40.7%) |
|
TSH: thyroid stimulating hormone; FNA: fine needle aspiration; MNG: multinodular goiter; GD: Graves’ disease; MFT: multifocal fibrosing thyroiditis; PTC: papillary thyroid carcinoma; CLND: central lymph node dissection |
|
Out of the 11 patients positive for PTC, tumor focality was predominantly unifocal, observed in 8 cases (72.7%), while multifocality was identified in 3 cases (27.3%). The mean tumor size among these 11 patients was 0.94 ± 0.88 cm, ranging from 0.2 to 3 cm. Postoperative serum thyroglobulin levels were available for 11 patients, all of which were ≤0.040 ng/ml (Table 3).
|
Variables |
Frequency |
|
Tumor size (cm), mean ± SD |
0.94 ± 0.88 |
|
Tumor Focality Unifocal Multifocal |
8 (72.7%) 3 (27.3%) |
|
Laterality Right lobe Left lobe Right lobe + isthmus Left lobe + isthmus |
7 (63.6%) 2 (18.2%) 1 (9.1%) 1 (9.1%) |
|
Post-operative thyroglobulin (ng/ml) ≤0.04 >0.04 |
11 (100.0%) 0 (0.0%) |
|
Lymphovascular invasion Present Not identified |
1 (9.1%) 10 (90.9%) |
|
Perineural invasion Seen Not seen |
0 (0.0%) 11 (100.0%) |
|
SD: standard deviation |
|
Discussion
Multifocal fibrosing thyroiditis continues to pose diagnostic and conceptual challenges, as its morphologic features may overlap with those of PTC, potentially leading to diagnostic confusion and overtreatment [1,3,9]. Clinically, patients with MFT most frequently present with thyroid nodules, though generalized weakness, thyroid function abnormalities, or incidental discovery during evaluation for other indications may also occur [1,9]. Given its often incidental identification in thyroidectomy specimens resected for unrelated indications, the true incidence and clinical significance of MFT remain incompletely defined [1,3].
The demographic characteristics of the current series are consistent with those of previously published series. In the study conducted by Fellegara G and Rosai J, 55 patients were evaluated, including 51 females (92.7%) and 4 males (7.3%), with ages ranging from 15 to 71 years and a mean age of 47.03 years [9]. Similarly, this series comprised 27 patients, of whom 22 (81.5%) were female, and 5 (18.5%) were male, with a mean age of 45.1 ± 8 years. Another study by Orsatti et al. included 7 patients, all of whom were female [1]. These findings collectively support a clear female predominance.
With regard to clinical presentation, the most common reason for seeking medical care in the current study was generalized body weakness, reported in 7 patients (25.9%). However, Fellegara G and Rosai J noted that detection of one or more thyroid nodules was the most frequent reason for medical evaluation [9]. Concerning thyroid functional status, in the current series, 3 patients (11.1%) had subclinical hypothyroidism and 4 patients (14.8%) had hyperthyroidism. In comparison, Fellegara G and Rosai J reported hyperthyroidism in 10 patients (18.2%) and hypothyroidism in 1 patient (1.8%) [9].
Surgical management in the current series predominantly involved total thyroidectomy, performed in 24 patients (88.9%). The remaining procedures included 1 left lobectomy (3.7%), 1 right partial lobectomy (3.7%), and 1 right lobectomy with right central lymph node dissection (3.7%). In contrast, Fellegara G and Rosai J reported that 29 patients (52.7%) underwent total thyroidectomy, 9 (16.3%) underwent right lobectomy, and 8 (14.6%) underwent left lobectomy [9].
One of the most important and debated aspects of MFT is its reported association with PTC. Although MFT is regarded as a benign fibroinflammatory process, multiple studies have documented its coexistence with PTC in a proportion of cases. In the current study, 11 patients (40.7%) were diagnosed with PTC. Similarly, Orsatti et al. reported an association rate of 38.5% between MFT and PTC [1]. In contrast, a study conducted by Frank et al. evaluated 7 cases in which both MFT and PTC were present and did not identify a close topographic relationship between fibrotic foci and carcinoma [3]. Furthermore, none of the MFT lesions showed BRAF mutations. Although they could not rule out the potential that MFT would be a very early step in the pathogenesis of PTC, the authors concluded that there was no indication of a pathogenetic link between MFT and PTC based on these data [3]. In the current series, among the 11 cases of PTC, 8 (72.7%) were unifocal, and 3 (27.3%) were multifocal. This distribution is comparable to that reported by Frank K et al., in which 5 of 7 cases (71.4%) were unifocal, and 2 (28.6%) were multifocal [3].
The pathogenesis of MFT remains incompletely understood and speculative. Several mechanisms have been proposed, including localized ischemic injury, autoimmune-mediated follicular damage, and a reparative response to repeated microtrauma [1]. The morphologic resemblance to radial scar type lesions in other organs has further prompted speculation that MFT may represent a patterned stromal response within a biologically susceptible thyroid gland [4,9,10]. Although the relatively high coexistence rate with PTC has raised concern regarding a potential preneoplastic role, available molecular data have not demonstrated clonal alterations within MFT lesions [1,3].
In our study, several limitations should be acknowledged. First, its retrospective design inherently introduces potential selection and information bias. Second, the details of the follow-up data were not sufficient. Third, molecular analysis was not performed in this study, preventing further exploration of potential pathogenetic mechanisms.
Conclusion
Multifocal fibrosing thyroiditis is a rare fibroinflammatory thyroid lesion that predominantly affects females and may coexist with PTC; therefore, accurate histopathologic recognition is essential to avoid diagnostic confusion and guide appropriate management. Further molecular and multicenter studies are needed to clarify the biological significance of this association.
Declarations
Conflicts of interest: The authors have no conflicts of interest to disclose.
Ethical approval: In accordance with our institution's oral policy, retrospective case series involving anonymized histopathological material and de-identified patient data do not require formal ethical approval.
Consent for participation: Not applicable.
Consent for publication: Informed consent for publication was obtained from the patients.
Funding: The present study received no financial support.
Acknowledgements: None to be declared.
Authors' contributions: AMS, KMS, SHA, IJH, and DAK: managed the cases, and performed critical revision. AMA and RMA: pathologists who contributed to the pathological analysis. AJQ: a radiologist who contributed to the radiological analysis. MHA and AAQ: contributed to conception of the idea, data collection and interpretation, and critical revision. AHA, MLF, and HAM: contributed to conception of the idea, literature review, table preparation, and critical revision. LLH: contributed to conception of the idea, literature review, and drafting of the manuscript. All authors have read and approved the final version of the manuscript.
Use of AI: ChatGPT-4.5 was used to assist with language refinement and improve the overall clarity of the manuscript. All content was thoroughly reviewed and approved by the authors, who bear full responsibility for the final version.
Data availability statement: Data are available from the corresponding author upon reasonable request.
References
- Orsatti A, De Leo A, Chiarucci F, Simoncini G, Cremonini N, Fornelli A, et al. Multifocal fibrosing thyroiditis: an under-recognized mimicker of papillary thyroid carcinoma. Endocrine Pathology. 2022 ;33(3):335-45. doi:10.1007/s12022-022-09726-0
- Rosai J, Carcangiu ML, DeLellis RA. Atlas of tumor pathology. Third series, fascicle 5. Washington (DC): Armed Forces Institute of Pathology; 1990. p. 310–311.
- Frank R, Baloch ZW, Gentile C, Watt CD, LiVolsi VA. Multifocal fibrosing thyroiditis and its association with papillary thyroid carcinoma using BRAF pyrosequencing. Endocrine pathology. 2014 ;25(3):236-40. doi:10.1007/s12022-013-9289-0
- Poli F, Trezzi R, Fellegara G, Rosai J. Multifocal sclerosing thyroiditis. International journal of surgical pathology. 2009 ;17(2):144. doi:10.1177/1066896908329800
- Jacobs TW, Byrne C, Colditz G, Connolly JL, Schnitt SJ. Radial scars in benign breast-biopsy specimens and the risk of breast cancer. New England Journal of Medicine. 1999 ;340(6):430-6. doi:10.1056/NEJM199902113400604
- Anderson TJ, Battersby S. Radial scars of benign and malignant breasts: comparative features and significance. The Journal of pathology. 1985 ;147(1):23-32. doi:10.1002/path.1711470104
- Abdullah HO, Abdalla BA, Kakamad FH, Ahmed JO, Baba HO, Hassan MN, et al. Predatory Publishing Lists: A Review on the Ongoing Battle Against Fraudulent Actions. Barw Med J. 2024;2(2):26-30. doi:10.58742/bmj.v2i2.91
- Goldblum JR, Lamps LW, McKenney JK, Myers JL, editors. Rosai and Ackerman's surgical pathology. 11th ed. Philadelphia: Elsevier; 2018.
- Fellegara G, Rosai J. Multifocal fibrosing thyroiditis: report of 55 cases of a poorly recognized entity. The American journal of surgical pathology. 2015 ;39(3):416-24. doi:10.1097/PAS.0000000000000337
- Fellegara G, Rosai J. Gross appearance of multifocal fibrosing thyroiditis. The American Journal of Surgical Pathology. 2015 ;39(6):870. doi:10.1097/PAS.0000000000000431

Copyright (c) 2026 The Author(s)

This work is licensed under a Creative Commons Attribution 4.0 International License.