Fine-Needle Aspiration Cytology and Salivary Gland Tumors: A Cross-Sectional Study

Abstract
Introduction
Salivary gland neoplasms are relatively rare and diverse, requiring accurate preoperative diagnosis. Although the Milan System for Reporting Salivary Gland Cytopathology (MSRSGC) has improved diagnostic consistency, fine-needle aspiration cytology (FNAC) performance remains variable. This study aims to assess FNAC’s diagnostic accuracy in salivary gland tumors and determinants affecting its performance.
Methods
This cross-sectional study was conducted at a tertiary care center and included patients with suspected salivary gland tumors. The FNAC was performed using a 22–24-gauge needle. All cases underwent histopathological examination. FNAC accuracy was assessed by comparing findings with final histopathological diagnosis, calculating sensitivity, specificity, positive predictive value, negative predictive value, and accuracy. Two diagnostic settings were defined based on MSRSGC categories
Results
Among 272 FNAC cases, 232 (85.3%) originated from the parotid gland. The mean patient age was 44.90 years, with 151 (55.5%) females. Histopathological examination identified 11 (4.0%) non-neoplastic lesions, 241 (88.6%) benign tumors, and 20 (7.4%) malignant tumors. FNAC sensitivity was 84.6% in Setting 1 and 88.2% in Setting 2. The FNAC success was significantly lower for submandibular gland lesions (OR = 0.218, p-value= 0.002).
Conclusion
Salivary gland FNAC is a minimally invasive, safe, and cost-effective diagnostic technique that may serve as an appropriate first-line investigation in the evaluation of major salivary gland lesions.
Introduction
Salivary gland neoplasms are relatively rare, with an annual incidence of 3.0 per 100,000 individuals [1]. These neoplasms account for approximately 6% of head and neck cancers and about 0.3% to 0.5% of all malignancies [2]. Primary salivary gland carcinomas constitute 20–35% of these cases, encompassing 21 clinically and biologically distinct entities [1,3]. Additionally, secondary salivary gland carcinomas, including metastatic solid tumors and lymphomas, may present in the lymph nodes of the parotid gland [1].
The risk of malignancy (ROM) associated with a salivary gland mass varies by its anatomical location. Specifically, it ranges from 20% to 25% for masses in the parotid gland, 40% to 50% in the submandibular gland, and 50% to 81% in the sublingual and minor salivary glands of the upper aerodigestive tract [4].
Given the wide variety of neoplasms affecting the salivary glands, a comprehensive and systematic diagnostic approach is essential to determine the most appropriate treatment. Preoperative differentiation between benign and malignant tumors is crucial for planning the extent of the surgical procedure [5]. However, imaging techniques alone have been shown to be insufficient in accurately distinguishing benign from malignant salivary gland tumors. Therefore, invasive preoperative diagnostic testing is often necessary. Both European and American guidelines for salivary gland neoplasms recommend the routine use of fine-needle aspiration cytology (FNAC) in the presence of a lesion in one of the major salivary glands, due to its simple application and low complication rates [6,7].
False diagnoses may occur when interpreting common neoplasms, such as pleomorphic adenoma and Warthin’s tumor. Moreover, a major challenge in FNAC is the possibility of obtaining unsatisfactory aspirates. Some specimens cannot be adequately assessed due to insufficient cellularity or poor quality, which can undermine the diagnostic accuracy. Immunostaining with Ki-67 fraction can be helpful in distinguishing malignant from benign tumors. Myoepithelial markers, such as S-100 and smooth muscle actin, are valuable for identifying the myoepithelial component, while markers like EMA and CEA assist in highlighting ductal structures [2].
The Milan System for Reporting Salivary Gland Cytopathology (MSRSGC), introduced in 2018, was developed to standardize cytopathological reports for salivary gland tumors and improve the accuracy of FNAC. While the MSRSGC has significantly enhanced diagnostic outcomes, performance measures for salivary gland FNAC remain controversial, with sensitivity ranging from 71% to 93% and specificity from 96% to 99% [1,8,9]. The factors influencing the success of FNAC, contributing to the broad variability in performance measures, remain largely unclear. Therefore, this study aims to evaluate the diagnostic role of FNAC in major salivary gland tumors and investigate factors influencing its accuracy. The references were assessed for eligibility [10].
Methods
Study Design and Setting
This cross-sectional study was carried out at a tertiary care hospital from March 2019 to December 2024 and patients were included consecutively based on their presentation over 5 years with clinically suspected salivary gland lesions.
Patient Selection and Data Collection
Patients included in the study with histopathologically confirmed benign or malignant salivary gland tumors. Exclusion criteria encompassed individuals with lesions of non-salivary gland origin, missing FNAC samples, and incomplete clinical or imaging data. Sociodemographic data, including age, sex, occupation, marital status, smoking status, and chief complaint, were collected. Additionally, relevant clinical details, including ultrasound tumor size, tumor size based on histopathology, side of involvement, FNAC findings, parotid involvement, type of operation, histopathology results, and follow-up information, were extracted and analyzed. All cases were classified according to the MSRSGC. The longest diameter (cm) of the lesion, as reported in the final pathology report, was used for analyses related to the lesion size.
Fine Needle Aspiration Cytology (FNAC)
The FNAC was performed for all enrolled patients with suspected salivary gland lesions. The procedure was conducted under ultrasound guidance using negative-pressure aspiration with a 22–24-gauge needle attached to a 10-cc syringe under aseptic conditions. For cystic lesions, the solid or mural component was targeted under aseptic conditions. For cystic lesions, the cyst was first aspirated and the lesion was then reassessed sonographically for any residual solid component; when a solid component was identified, immediate re-aspiration of that component was performed, with material preferentially collected for cell block preparation to optimize cellular yield. Aspirated material was immediately smeared onto glass slides, and each specimen was gently spread between two slides to obtain adequate cytological preparations. When sufficient material was available, the residual specimen was processed for cell block preparation, also stained with hematoxylin and eosin, to facilitate further histopathological assessment and ancillary studies. Immunocytochemistry was used when the cytological diagnosis was inconclusive or required further confirmation. Specimen adequacy required both sufficient cellularity (quantitative) and lesional representativeness (qualitative); a specimen was considered adequate when it contained well-preserved lesional cells, whereas aspirates showing only obscuring artifact, non-mucinous cyst fluid without epithelial cells, or normal salivary tissue from a targeted mass were classified as non-diagnostic. Non-diagnostic specimens were repeated, either on the same day or at a subsequent visit.
Histopathological Examination
Following FNAC, all patients underwent surgical excision of the lesion, and the resected tissue was sent for histopathological examination. The specimens were fixed in 10% formalin, routinely processed, and embedded in paraffin. Serial sections were cut and stained with hematoxylin and eosin. Special histochemical stains were applied at the discretion of the reporting pathologist in defined scenarios: periodic acid-Schiff with diastase (PAS-D) to confirm diastase-resistant mucin in lesions suspected of mucoepidermoid carcinoma and to demonstrate zymogen granules where acinic cell carcinoma was in the differential; PAS to highlight basement-membrane-like material in basaloid or cribriform lesions suspected of adenoid cystic carcinoma and to identify glycogen in clear-cell lesions; and PAS to screen for fungal organisms in cases of granulomatous inflammation. Final diagnoses were based on hematoxylin and eosin morphology supplemented by immunohistochemistry where indicated, with special stains serving only as confirmatory adjuncts.
Statistical Analysis
The diagnostic performance of FNAC was evaluated by comparing its findings with the histopathological diagnoses. Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and diagnostic accuracy were calculated. In accordance with a previous study [9], two settings were defined for calculating the performance measures. In Setting 1, the MSRSGC categories V and VI, which correspond to 'suspicious for malignancy' and 'malignant' respectively, were considered as positive index tests. Conversely, MSRSGC categories II and IVa, representing 'non-neoplastic' and 'neoplasm-benign', were classified as negative tests. In Setting 2, MSRSGC categories III, IVb, V, and VI, encompassing 'atypia of undetermined significance (AUS)', 'salivary gland neoplasm of uncertain malignant potential (SUMP)', 'suspicious for malignancy', and 'malignant', were designated as positive index tests. Similarly, MSRSGC categories II and IVa were maintained as negative tests. FNAC was considered successful when the specimen was adequate for cytological interpretation, corresponding to MSRSGC categories II–VI. Conversely, FNAC was classified as unsuccessful when the result was non-diagnostic, consistent with MSRSGC category I. Data analysis was performed using SPSS software (version 26.0). Univariate logistic regression was employed to identify factors influencing the success of FNAC. A p-value of <0.05 was considered statistically significant.
Results
A total of 272 salivary gland FNAC cases were included. Among these, 232 (85.3%) originated from the parotid gland, while 40 (14.7%) involved the submandibular gland. The patient cohort had a mean age of 44.90±15.0 years, with 151 (55.5%) being female (Table 1).
|
Variables |
N, Mean (%, SD) |
|
Age |
44.90±15.0 |
|
Age group 10-20 20-30 30-40 40-50 50-60 60-70 70-80 >80 |
16 (5.9) 32 (11.8) 64 (23.5) 59 (21.7) 61 (22.4) 28 (10.3) 10 (3.7) 2 (0.7) |
|
Gender Male Female |
1 (9.1%) 121 (44.5) 151 (55.5) |
|
Marital Status Single Widow Married |
37 (13.6) 1 (0.4) 234 (86.0) |
|
Smoking Status Non-smoker Active Passive Ex-smoker |
191 (70.2) 59 (21.7) 20 (7.4) 2 (0.7) |
|
Side Right Left Bilateral |
134 (49.3) 136 (50.0) 2 (0.7) |
|
Gland Parotid gland Submandibular gland |
232 (85.3) 40 (14.7) |
|
Type of operation Superficial parotidectomy Submandibular gland excision Total parotidectomy Submandibular gland excision + Neck dissection Parotid gland excision |
211 (77.6) 35 (12.9) 19 (7.0) 5 (1.8) 2 (0.7) |
|
Tumor size (Longest dimension) (cm) |
2.56±1.17 |
|
Follow-up Normal Dead |
271 (99.6) 1 (0.4) |
The most common category was MSRSGC IVa (neoplasm-benign), accounting for 223 (82.0%) of cases. The highest risk of neoplasm was observed in MSRSGC categories IVb (SUMP), III (AUS), and VI (malignant), each demonstrating a rate of 100.0%. In contrast, the lowest risk of neoplasm was recorded in MSRSGC II (non-neoplastic) cases, at 0.0%. Regarding the ROM, MSRSGC VI (malignant) cases showed a rate of 100.0%, whereas MSRSGC II (non-neoplastic) and MSRSGC IVa (benign neoplasm) demonstrated ROM values of 0.0% and 0.9%, respectively (Table 2).
|
Category |
Final Diagnosis |
Total n, (%) |
RON (%) |
ROM (%) |
||
|
Non-neoplastic |
Benign |
Malignant |
||||
|
Non-diagnostic, I |
4 |
13 |
3 |
20 (7.4) |
80.0 |
15.0 |
|
Non-Neoplastic, II |
1 |
0 |
0 |
1 (0.4) |
0.0 |
0.0 |
|
AUS, III |
0 |
5 |
1 |
6 (2.2) |
100.0 |
16.7 |
|
Neoplasm-benign, IVa |
5 |
216 |
2 |
223 (82.0) |
97.8 |
0.9 |
|
Neoplasm-SUMP, IVb |
0 |
7 |
3 |
10 (3.7) |
100.0 |
30.0 |
|
SFM, V |
1 |
0 |
7 |
8 (2.9) |
87.5 |
87.5 |
|
Malignant, VI |
0 |
0 |
4 |
4 (1.5) |
100.0 |
100.0 |
|
Total |
11 |
241 |
20 |
272 (100.0%) |
96.0 |
7.4 |
|
M:Male, F:Female, S.Ca:Serum calcium, TG:Thyroglobulin, N/A:Not applicable |
||||||
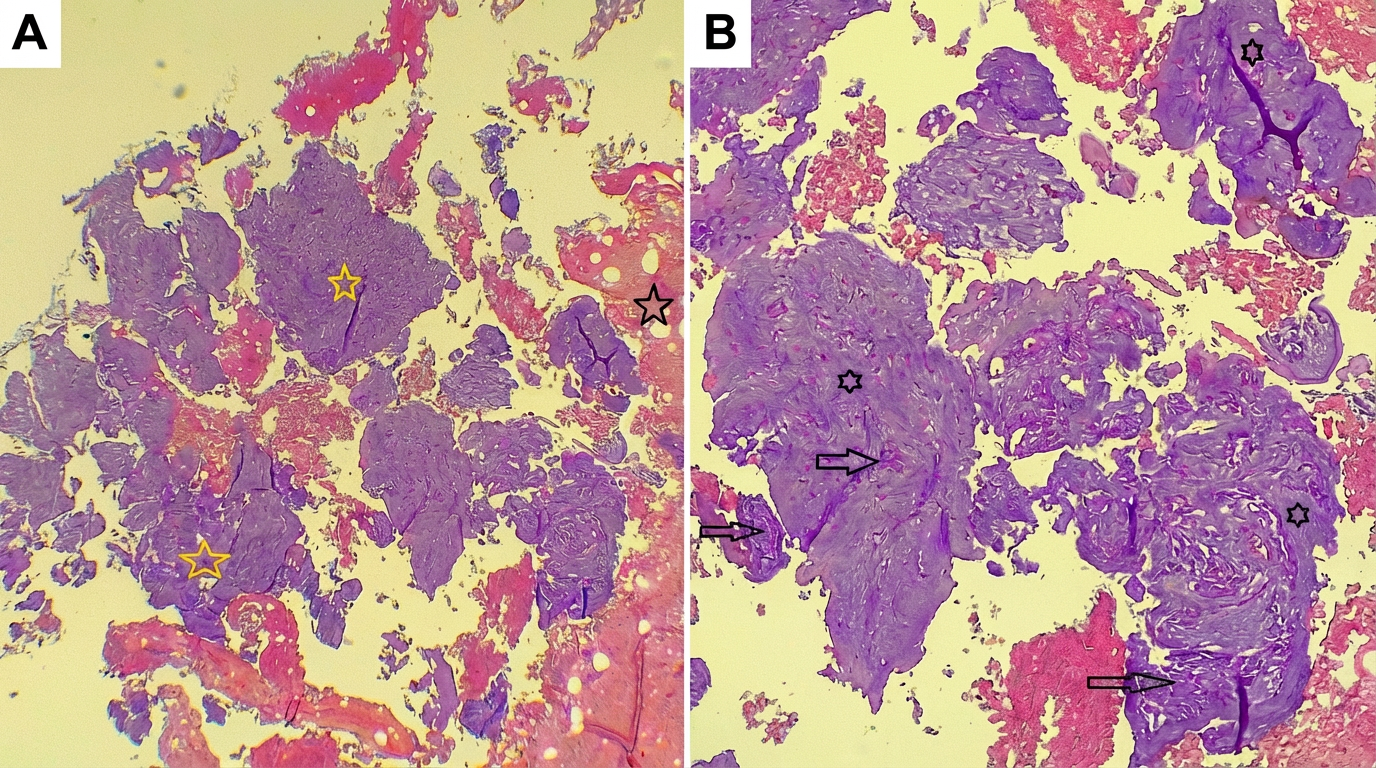
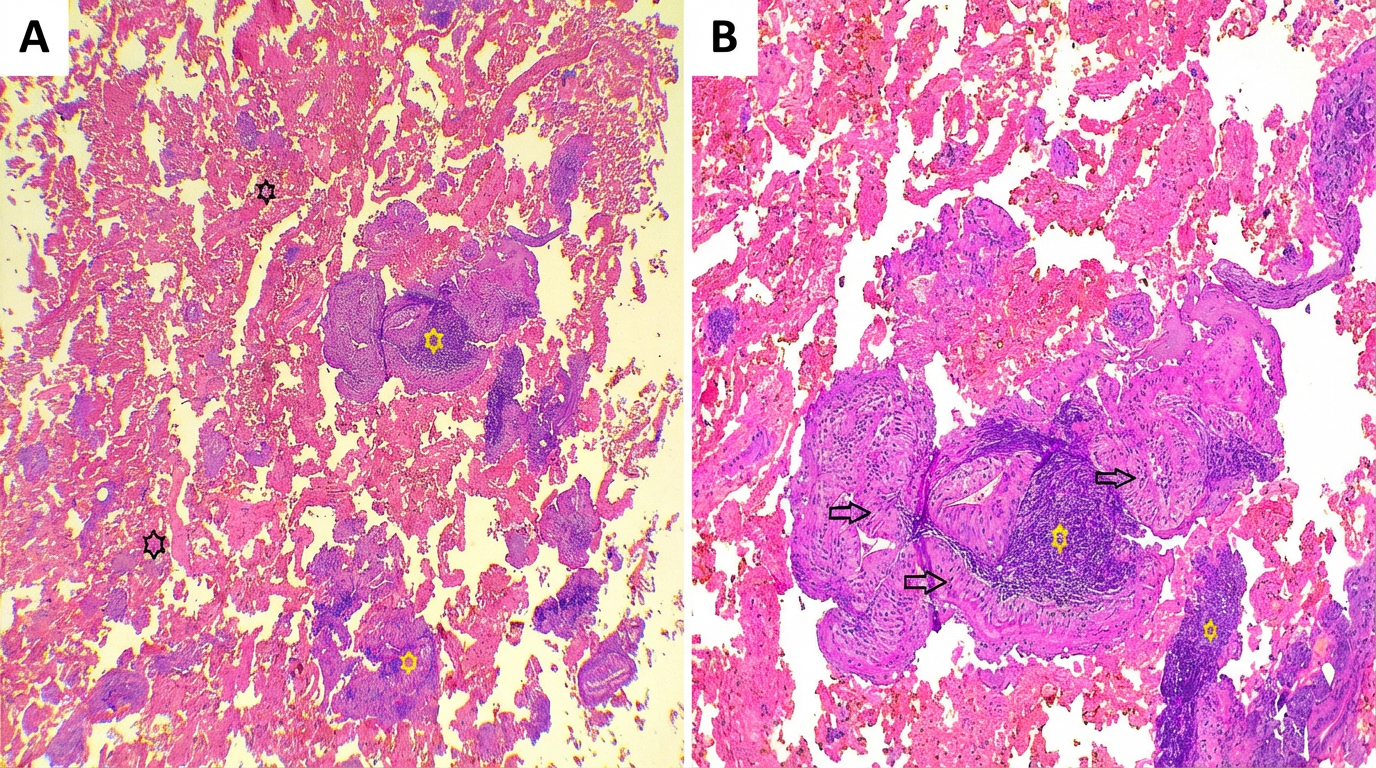
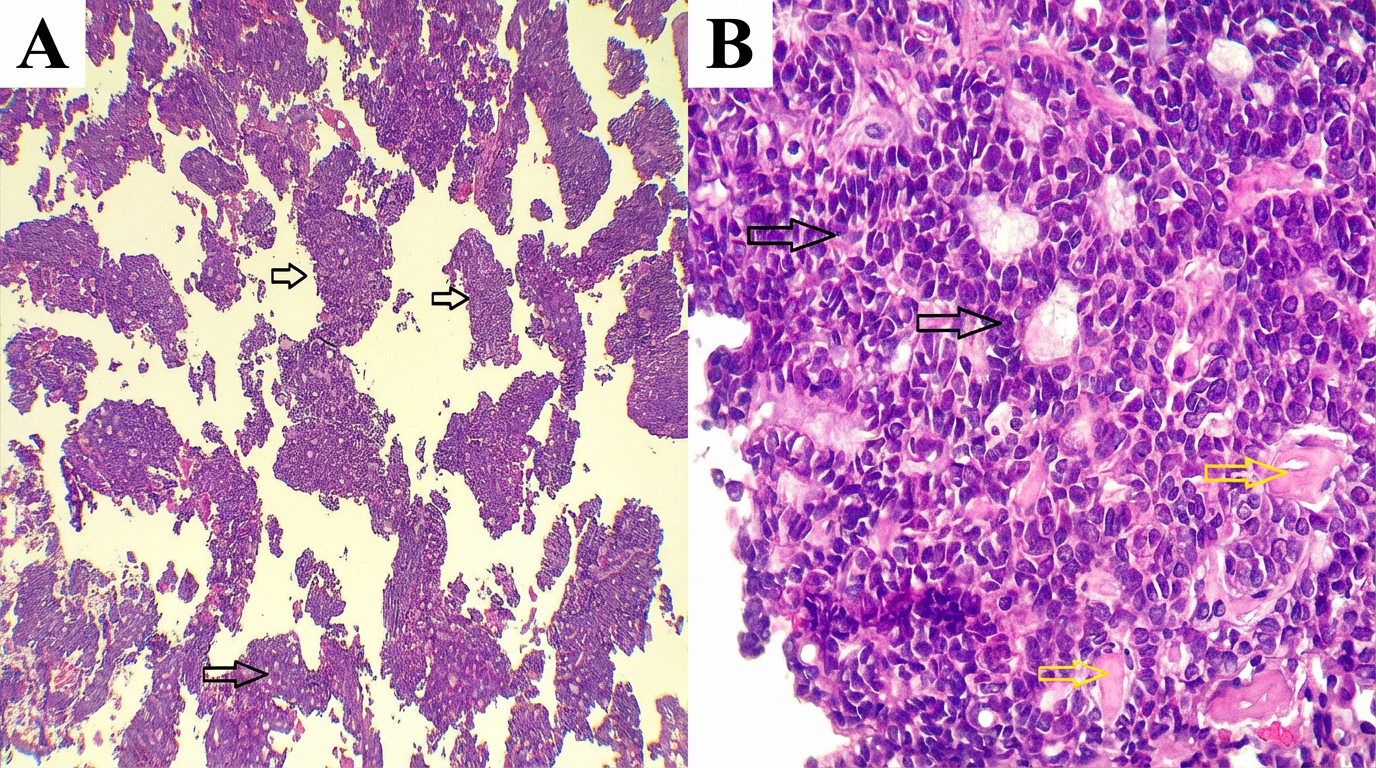
Histopathological follow-up revealed 11 (4.0%) cases of non-neoplastic lesions, 241 (88.6%) cases of benign tumors, and 20 (7.4%) cases of malignant tumors. Among the benign tumors, pleomorphic adenoma was the most common entity, identified in 169 (62.1%) cases, followed by Warthin tumor in 47 (17.3%) cases (Figures 1 and 2). Regarding malignant tumors, mucoepidermoid carcinoma was the most frequently diagnosed subtype, accounting for 8 (2.9%) cases, followed by squamous cell carcinoma in 3 (1.1%) cases and adenoid cystic carcinoma in 2(0.7%) cases (Figure 3) (Table 3).
|
Lesions |
Number of cases (%) |
|
Non-neoplastic |
11 (4.0) |
|
Sialadenitis |
8 (2.9) |
|
Lymphoepithelial Cyst |
2 (0.7) |
|
Lymphoid Hyperplasia |
1 (0.4) |
|
Neoplastic |
4 (36.3%) |
|
Benign tumors |
241 (88.6) |
|
Pleomorphic Adenoma |
169 (62.1) |
|
Warthin Tumor |
47 (17.3) |
|
Oncocytoma |
8 (0.4) |
|
Benign Salivary Gland Tissue |
4 (1.5) |
|
Vascular Hamartoma |
3 (1.1) |
|
Basal Cell Adenoma |
2 (0.7) |
|
Canalicular Adenoma |
2 (0.7) |
|
Giant Cell Tumor |
2 (0.7) |
|
Myoepithelioma |
1 (0.4) |
|
Lipoma |
1 (0.4) |
|
Schwannoma |
1 (0.4) |
|
Intra-parotid Cavernous Hemangioma |
1 (0.4) |
|
Malignant tumors |
20 (7.4) |
|
Mucoepidermoid Carcinoma |
8 (2.9) |
|
Squamous Cell Carcinoma |
3 (1.1) |
|
Adenoid Cystic Carcinoma |
2 (0.7) |
|
Adenocarcinoma |
1 (0.4) |
|
Salivary Duct Carcinoma |
1 (0.4) |
|
Epithelial-Myoepithelial Carcinoma |
1 (0.4) |
|
Mammary Analogue Secretory Carcinoma |
1 (0.4) |
|
Non-Hodgkin’s Lymphoma |
1 (0.4) |
|
Acinic Cell Carcinoma |
1 (0.4) |
|
Basaloid Cell Carcinoma |
1 (0.4) |
In setting 1, for distinguishing malignant from benign tumors, which excluded tumors classified as AUS and SUMP, the diagnostic performance was as follows: sensitivity 84.6%, specificity 99.6%, accuracy 98.7%, PPV 91.7%, and NPV 99.1%. In Setting 2, which included AUS and SUMP cases, the sensitivity increased to 88.2%, while specificity, accuracy, PPV, and NPV were 94.5%, 94.1%, 53.6%, and 99.1%, respectively (Table 4).
|
Setting |
Sensitivity, % |
Specificity, % |
Accuracy, % |
PPV, % |
NPV, % |
|
Setting 1 |
84.6 |
99.6 |
98.7 |
91.7 |
99.1 |
|
Setting 2 |
88.2 |
94.5 |
94.1 |
53.6 |
99.1 |
|
PPV: positive predictive value, NPV: negative predictive value |
|||||
Regression analysis showed that tumor size was not a statistically significant predictor of FNAC success; however, it was associated with an increased odds of successful FNAC, with each additional centimeter corresponding to a 50% increase in the odds of success (OR = 1.50). In contrast, FNAC success was significantly lower for lesions located in the submandibular gland compared with the parotid gland (OR = 0.218, 95% CI: 0.083–0.575; p-value= 0.002) (Table 5).
|
Variable |
B (SE) |
OR (95% CI) |
p-value |
|
Tumor size (cm) |
0.405 (0.254) |
1.500 (0.911–2.469) |
0.111 |
|
Gland Parotid gland Submandibular gland |
-1.522 (0.494) |
1 0.218 (0.083-0.575) |
0.002 |
|
B: Logistic regression coefficient, SE: Standard error, OR: Odds ratio, CI: confidence interval |
|||
Discussion
Fine-needle aspiration is a safe, minimally invasive, and cost-effective diagnostic modality widely used for the preoperative evaluation of lesions across various organs. However, its diagnostic utility in salivary gland lesions remains a subject of ongoing debate [11]. Salivary gland neoplasms can occur across a broad age range. A study by Rameeza et al., which included 104 patients, reported a mean age of 45 years, with peak incidence in the fourth decade of life [11]. Similarly, Kakoty et al. also identified the fourth decade as the most affected age group [12]. In contrast, studies conducted by Koirala et al. and Omhare et al. found a higher incidence in the third decade [13,14]. In the present study, the mean age was 44.90 years, with the highest prevalence observed in the fourth decade of life, consistent with the findings of previous reports.
Studies examining the role of FNAC in diagnosing salivary gland tumors have demonstrated variability in sex distribution. A ten-year retrospective study from Greece reported a male predominance, with a male-to-female ratio of 1.28:1 (46 males vs. 36 females) [15]. Similarly, a systematic review of 45 cases of secretory carcinoma also demonstrated a male predominance, with 25 (55.6%) males and 20 (44.4%) females [16]. Conversely, other investigations have described either a balanced or female-predominant distribution. An analysis of 37 FNAC specimens demonstrated an equal gender distribution (17 males vs. 20 females) [17]. Likewise, a study of 81 cases reported a slight female predominance, with 51.85% of cases occurring in females, corresponding to a male-to-female ratio of 1:1.33 [18]. In this study, comprising 272 cases, a slight female predominance was observed, with 55.5% of cases occurring in females, yielding a male-to-female ratio of 1:1.25.
The relative proportions of benign, malignant, and non-neoplastic salivary gland tumors vary across published series. A large study from Southern Iran involving 405 cases reported that 74.5% were benign and 25.4% malignant. The most frequently observed benign tumors were pleomorphic adenoma (70.5%) and Warthin’s tumor (21.5%), whereas mucoepidermoid carcinoma (26.2%) and adenoid cystic carcinoma (22.3%) predominated among malignant tumors. Additionally, the study found that benign tumors predominantly affected the parotid gland and were more common in younger individuals, whereas malignant tumors were more frequently observed in older age groups [19]. Similarly, an analysis of 318 patients with primary salivary gland carcinomas identified adenoid cystic carcinoma, mucoepidermoid carcinoma, and squamous cell carcinoma as the most prevalent malignant entities, with the parotid gland being the most commonly affected site [20]. Another study of 124 cases found benign neoplasms in 31.45% (39 cases) and malignant tumors in 15.32% of cases, with pleomorphic adenoma and mucoepidermoid carcinoma representing the most common benign and malignant entities, respectively; 68.9% of neoplasms arose in the parotid gland [14]. In the current study, benign tumors accounted for 88.6% of cases, while 7.4% were malignant. The lower proportion of malignant tumors observed in this cohort compared with several published series may be attributable to differences in referral patterns, patient selection, and the predominance of parotid gland lesions, which are more likely to be benign than lesions arising in other major salivary glands. This distribution may have contributed to the relatively high specificity and negative predictive value observed in the present study and should be considered when interpreting the diagnostic performance of FNAC. Additionally, pleomorphic adenoma was the most prevalent benign tumor in this study, followed by Warthin’s tumor, whereas among malignant neoplasms, mucoepidermoid carcinoma was the most common, followed by squamous cell carcinoma. Additionally, the parotid gland was identified as the most frequently affected site, accounting for about 85.3% of cases.
In this study, the ROM for MSRSGC category I (non-diagnostic) was 15.0%, consistent with the 15% benchmark recommended in the second edition of the MSRSGC [21]. This rate exceeds the 11.4% reported in the large meta-analysis by Wang et al., which analyzed 7,168 FNAC cases [9], and is also higher than the 3.2% inadequacy rate observed in the study by Kim et al., where salivary gland FNAC were performed by a single radiologist with six years of experience [22]. However, the current study ROM remains lower than the 23.9% reported in another series [1]. In contrast, among 223 cases classified as MSRSGC category IVa (benign neoplasm), the ROM was merely 0.9%, which is lower than the 2.8% reported in Wang et al.'s meta-analysis [9], and comparable to the 1.0% documented in another study [1]. These findings further support the high diagnostic accuracy and reliability of FNAC when adequate sampling and expert cytological interpretation are achieved.
The FNAC is integral to the preoperative assessment of salivary gland tumors, offering a minimally invasive and cost-effective approach to differentiate benign from malignant lesions. Nevertheless, reported diagnostic performance varies across studies. A large series of 1,289 cases evaluated FNAC in two diagnostic settings and demonstrated sensitivity and specificity of 87.5% and 97.7% in one setting, and 91.6% and 81.6% in the other, underscoring its overall reliability while highlighting the potential for false-positive results [1]. Similarly, Naz et al. reported a sensitivity of 77.7% and specificity of 86.3%, reflecting moderate effectiveness in detecting malignancy and relatively higher accuracy in confirming benign disease [23]. Despite its utility, FNAC exhibits limitations in certain histological subtypes. A 2024 systematic review and meta-analysis reported a notably low sensitivity of 27.7% (95% CI: 16.6–42.5%) for secretory carcinoma, largely due to significant cytomorphological overlap with other benign and malignant entities; FNAC alone provided a definitive diagnosis in only 6.6% of cases, emphasizing the need for adjunctive diagnostic modalities [16]. Likewise, Kim et al. documented a sensitivity of 64.2% for high-grade salivary gland malignancies, illustrating the challenges in accurately distinguishing aggressive tumors from benign lesions in complex scenarios [22]. In the present study, FNAC performance was assessed in two analytical settings.
When only definitive cytological diagnoses were considered (Setting 1), sensitivity and specificity were 84.6% and 99.6%, respectively. Inclusion of indeterminate categories (Setting 2) yielded sensitivity and specificity of 88.2% and 94.5%, respectively. Variations in diagnostic accuracy across studies likely reflect differences in tumor heterogeneity, cytopathologist expertise, specimen adequacy, case mix, and institutional protocols.
A large single-center study from Germany identified lesion size as an independent predictor of sample adequacy in salivary gland FNAC, reporting a 22% increase in diagnostic success for each additional centimeter in lesion diameter [1]. In contrast, another investigation found no significant association between tumor size and FNAC success [22]. Conversely, a separate study demonstrated that sensitivity, specificity, and overall accuracy were higher in parotid lesions measuring 2.1–4.0 cm compared with those smaller than 2 cm [24]. In the present study, although lesion size did not reach statistical significance, it was associated with improved adequacy, with each additional centimeter increasing the odds of successful FNAC by 50%.
Regarding lesion location, the aforementioned German study reported significantly lower FNAC success rates for submandibular gland lesions compared with parotid lesions [1]. By contrast, Kim et al. did not observe a significant relationship between gland location and diagnostic performance, possibly reflecting their smaller sample size [22]. The current study’s finding aligns with the German data, demonstrating significantly reduced FNAC success in the submandibular gland relative to the parotid gland. This discrepancy may be explained by the submandibular gland’s deeper anatomical position within the submandibular triangle, which can limit accessibility and compromise sampling. Collectively, these results underscore the importance of meticulous technique and careful procedural planning when performing FNAC in anatomically challenging regions.
This study has several limitations that warrant consideration. First, its retrospective design inherently introduces potential selection and information biases, which may affect the interpretation of the findings. Second, the exact number of needle passes performed during each FNAC procedure was not consistently documented. Although institutional protocol generally recommends a single-pass technique, the possibility that additional passes were undertaken in selected cases cannot be excluded. Future prospective studies with standardized procedural documentation are needed to clarify the impact of the number of needles passes on sample adequacy and diagnostic accuracy in salivary gland FNAC.
Conclusion
Salivary gland FNAC is a minimally invasive, safe, and cost-effective diagnostic technique that may serve as an appropriate first-line investigation in the evaluation of major salivary gland lesions.
Declarations
Conflicts of interest: The authors have no conflicts of interest to disclose.
Ethical approval: As the study design was a retrospective cohort study based on the analysis of existing clinical records, formal ethical approval was not required in accordance with institutional policy.
Consent for participation: Not applicable.
Consent for publication: Written informed consent for publication was obtained from all patients or from their legal guardians in cases involving minors.
Funding: The present study received no financial support.
Acknowledgements: None to be declared.
Authors' contributions: AJQ, AMA, KMS, and AMM: Major contributors to the conception and design of the study, literature review, and manuscript writing. STA, MLF, HAM, ISS, IJH, MBA, RSA, SHQ, AAQ, SHH, and HAA: Literature review, critical revision of the manuscript, and preparation of the tables and figures. All authors have read and approved the final version of the manuscript.
Use of AI: ChatGPT-4.5 was used to assist with language refinement and improve the overall clarity of the manuscript. All content was thoroughly reviewed and approved by the authors, who bear full responsibility for the final version.
Data availability statement: The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
- Mayer M, Alfarra MM, Möllenhoff K, Engels M, Arolt C, Quaas A, et al. The Impact of Lesion-Specific and Sampling-Related Factors on Success of Salivary Gland Fine-Needle Aspiration Cytology. Head and Neck Pathology. 2025;19(1):1. doi:10.1007/s12105-024-01741-3
- Sarkar A, Sharma N, Sharma S. Fine needle aspiration cytology utility in salivary gland tumor diagnosis. Indian Journal of Otolaryngology and Head & Neck Surgery. 2017; 69:147-54. doi:10.1007/s12070-016-0982-4
- Alsanie I, Rajab S, Cottom H, Adegun O, Agarwal R, Jay A, et al. Distribution and frequency of salivary gland tumours: an international multicenter study. Head and neck pathology. 2022;16(4):1043-54. doi:10.1007/s12105-022-01459-0
- Pusztaszeri M, Rossi ED, Faquin WC. Update on salivary gland fine-needle aspiration and the Milan System for Reporting Salivary Gland Cytopathology. Archives of Pathology & Laboratory Medicine. 2024;148(10):1092-104. doi:10.5858/arpa.2022-0529-RA
- Qaradakhy AJ, Ali RM, Ali RM, Salih AM, Rashid RJ, Hassan SH, et al. Hodgkin lymphoma of the parotid gland: A case report with literature review. Acta Oto-Laryngologica Case Reports. 2025;10(1):18-25. doi:10.1080/23772484.2025.2466616
- van Herpen C, Vander Poorten V, Skalova A, Terhaard C, Maroldi R, van Engen A, et al. Salivary gland cancer: ESMO–European Reference Network on Rare Adult Solid Cancers (EURACAN) clinical practice guideline for diagnosis, treatment and follow-up. ESMO open. 2022;7(6):100602. doi:10.1016/j.esmoop.2022.100602
- Geiger JL, Ismaila N, Beadle B, Caudell JJ, Chau N, Deschler D, et al. Management of salivary gland malignancy: ASCO guideline. Journal of Clinical Oncology. 2021;39(17):1909-41. doi:10.1200/JCO.21.00449
- Rossi ED, Baloch ZW, Pusztaszeri M, Faquin WC. The Milan System for Reporting Salivary Gland Cytopathology (MSRSGC): an ASC-IAC-sponsored system for reporting salivary gland fine-needle aspiration. Acta Cytologica. 2018;62(3):157-65. doi:10.1159/000488969
- Wang Z, Zhao H, Guo H, An C. Application of the Milan System for Reporting Salivary Gland Cytopathology: a systematic review and meta‐analysis. Cancer Cytopathology. 2022;130(11):849-59. doi:10.1002/cncy.22604
- Fahmi H. Kakamad, Shvan H. Mohammed, Berun A. Abdalla, Dahat A. Hussein, Zuhair D. Hammood, Suhaib H. Kakamad, et al. Non-Recommended Publishing Lists: Strategies for Detecting Deceitful Journals. Barw Medical Journal. 2026;4(1):13-21. doi:10.58742/bmj.v4i1.227
- Rameeza A, Hemalata M. Fine-needle aspiration cytology of salivary gland lesions. Journal of Oral and Maxillofacial Pathology. 2022;26(1):52-6. doi:10.4103/jomfp.jomfp_496_20
- Kakoty S, Baruah TD, Babu CG. FNAC and histopathological correlation of salivary gland lesions: an observational study. Int surg J. 2017;4(7):2148-52. doi:10.18203/2349-2902.isj20172624
- Koirala S, Sayami G, Pant AD. Correlation of FNAC and histopathology in diagnosis of salivary gland lesions. Journal of Pathology of Nepal. 2014;4(8):654-7. doi:10.3126/jpn.v4i8.11593
- Omhare A, Singh SK, Nigam JS, Sharma A. Cytohistopathological study of salivary gland lesions in Bundelkhand region, Uttar Pradesh, India. Pathology research international. 2014;2014(1):804265. doi:10.1155/2014/804265
- Mourouzis C, Schoinohoriti O, Mastagkas D, Rallis G. Fine-needle aspiration cytology in the diagnosis of salivary gland tumors before the Milan System: a ten-year experience from a Tertiary Care Center in Greece. Cureus. 2023;15(7):e42737. doi:10.7759/cureus.42737
- Kala PS, Gupta M, Thapliyal N. Efficacy of Fine-Needle Aspiration Cytology in Diagnosing Secretory Carcinoma of Salivary Gland: A Systematic Review and Meta-Analysis. Acta Cytologica. 2024;68(2):83-106. doi:10.1159/000536249
- AlGhamdi GZ, Alzahrani AK, Saati H, Algarni HM, Alshehri KA, Baroom M, et al. Correlation between fine needle aspiration cytology (FNAC) and permanent histopathology results in salivary gland masses. Cureus. 2021;13(3):e13976. doi:10.7759/cureus.13976
- Poudel A, Shrestha B, Regmi S. Evaluation of salivary gland lesions by fine needle aspiration cytology at a tertiary care hospital, Western Nepal. Pathology and Laboratory Medicine International. 2020;12:9-17. doi:10.2147/PLMI.S266866
- Ghaderi H, Kruger E, Ahmadvand S, Mohammadi Y, Khademi B, Ghaderi A. Epidemiological profile of salivary gland tumors in Southern Iranian population: a retrospective study of 405 cases. Journal of Cancer Epidemiology. 2023;2023(1):8844535. doi:10.1155/2023/8844535
- Nachtsheim L, Jansen L, Shabli S, Arolt C, Quaas A, Klussmann JP, et al. Recurrence after primary salivary gland carcinoma: Frequency, survival, and risk factors. Head & Neck. 2025;47(1):47-56. doi:10.1002/hed.27880
- Baloch Z, Lubin D, Katabi N, Wenig BM, Wojcik EM. The Milan system for reporting salivary gland cytopathology. InThe Milan System for Reporting Salivary Gland Cytopathology 2023. Cham: Springer International Publishing. doi:10.1007/978-3-031-26662-1_1
- Kim MW, Kim DW, Jung HS, Choo HJ, Park YM, Jung SJ, et al. Factors influencing the outcome of ultrasound‐guided fine‐needle aspiration for salivary gland lesion diagnosis. Journal of Ultrasound in Medicine. 2016;35(5):877-83. doi:10.7863/ultra.15.06062
- Naz S, Hashmi AA, Khurshid A, Faridi N, Edhi MM, Kamal A, et al. Diagnostic role of fine needle aspiration cytology (FNAC) in the evaluation of salivary gland swelling: an institutional experience. BMC research notes. 2015;8:1-5. doi:10.1186/s13104-015-1048-5
- Altin F, Alimoglu Y, Acikalin RM, Yasar H. Is fine needle aspiration biopsy reliable in the diagnosis of parotid tumors? Comparison of preoperative and postoperative results and the factors affecting accuracy. Brazilian journal of otorhinolaryngology. 2019; 85:275-81. doi:10.1016/j.bjorl.2018.04.015

Copyright (c) 2026 The Author(s)

This work is licensed under a Creative Commons Attribution 4.0 International License.