Video-Assisted Thoracoscopic Surgery for Bilateral Giant Pulmonary Hydatid Cysts: A Case Report and Literature Review

Abstract
Introduction: Bilateral giant pulmonary hydatid cysts (HCs) are rare but can lead to serious respiratory complications. Despite growing interest in minimally invasive surgery, the role of Video-Assisted Thoracoscopic Surgery (VATS) in their management remains controversial. This report describes a case of giant bilateral pulmonary HCs managed using a VATS approach.
Case presentation: A 34-year-old male presented with chest discomfort, productive cough, and exertional dyspnea. Imaging revealed bilateral giant pulmonary HCs, including an uncomplicated cyst in the right upper lobe and a ruptured, infected cyst in the left lower lobe. The patient underwent single-session bi-port VATS with cyst evacuation, hypertonic saline irrigation, and closure of bronchopleural fistulae. Intraoperative culture grew Pseudomonas aeruginosa, and the patient received albendazole and culture-directed antibiotics, resulting in an uneventful recovery.
Literature review: Among 12 reviewed cases of pulmonary HCs, patients’ ages ranged from 3 to 42 years, with a predominance of males (7/12). Cough was present in all cases, while dyspnea and fever were reported in 50% of the cases. Bilateral cysts were documented in 6 cases. Management included VATS alone in 5 cases, thoracotomy-based surgery in 4, hybrid approaches in 2, and conservative treatment in 1. Complications occurred in 2 cases. Albendazole therapy was administered postoperatively in 7 cases, and overall outcomes were positive, with 11 patients experiencing uneventful recovery.
Conclusion: Bilateral VATS in a single session may be a feasible therapeutic approach for giant pulmonary HCs, even when complicated cysts are present.
Introduction
Echinococcosis is a widely recognized zoonotic disease caused by the larval form of the tapeworm Echinococcus granulosus [1]. Although the disease can occur globally, it is considered endemic in several regions, including the Middle East, the Mediterranean basin, parts of South America, South Africa, and Australia [1]. Humans serve as accidental intermediate hosts for the parasite, acquiring the infection through direct contact with definitive hosts (such as dogs) or via ingestion of food or water contaminated with feces that contain parasitic eggs, often originating from livestock environments involving sheep, goats, or cattle [2]. Major risk factors include close contact with dogs, involvement in livestock activities, and living in endemic areas [2]. The prevalence of hydatid cysts in children differs by region, with a reported incidence of 2-6 cases per 100,000 children affecting individuals as young as six months old. Human infections typically occur incidentally through the ingestion of parasite eggs in contaminated food or water or by direct contact with infected hosts [3,4]. Hydatid cysts (HCs) are typically found in the liver and lungs, while the adrenal gland is a rare and unusual site of involvement [5]. This report presents a case of a primary adrenal HC (AHC) that was incidentally diagnosed in a child. The references cited in this report have been reviewed to ensure the exclusion of any non-peer-reviewed data, and the study has been structured following the CaReL guidelines [6,7].
Case presentation
Patient information
A 34-year-old non-smoking male from an urban area presented with a 15-day history of chest discomfort and productive cough, accompanied by dyspnea on exertion. He denied fever, rigors, or hemoptysis. There was no history of contact with dogs or cattle, and no family history of hydatid disease. His past medical and surgical history was unremarkable.
Clinical findings
On physical examination, the patient was afebrile and hemodynamically stable. Chest auscultation revealed decreased air entry bilaterally.
Diagnostic approach
Hematological analysis showed leukocytosis with a white blood cell count of 14.3 × 10⁹/L (Normal range: 4.5–11.0 × 10⁹/L). Inflammatory markers were markedly elevated, with an ESR (erythrocyte sedimentation rate) of 100 mm/hr (Normal range: 0–15 mm/hr) and CRP of 237 mg/dL (Normal range: <1.0 mg/dL). Chest radiography revealed a well-defined opacity in the right upper zone and a cavitary lesion in the left lower zone (Figure 1).

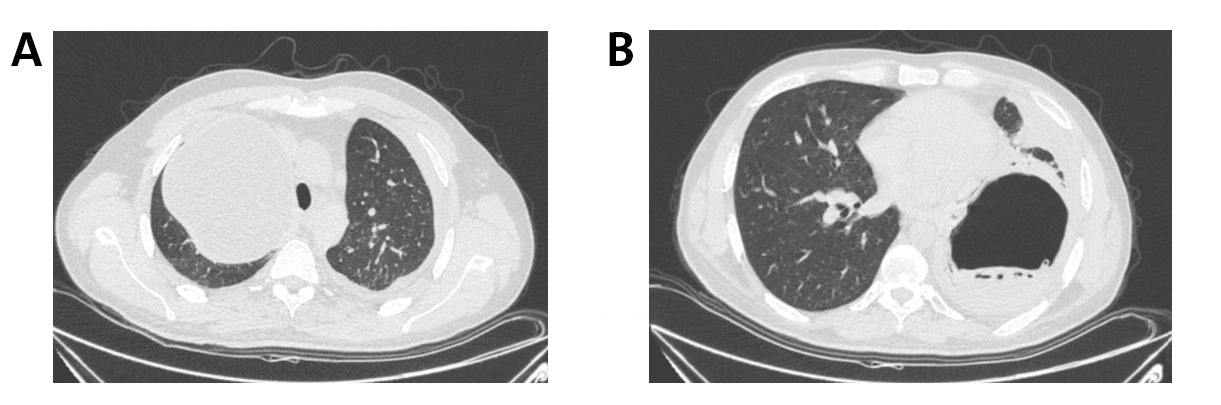
Contrast-enhanced computed tomography (CT) confirmed the presence of bilateral giant cysts suggestive of HCs. The right upper lobe contained a large, uncomplicated HC measuring 14 × 12 × 11 cm, associated with mild adjacent atelectasis. In addition, a complicated (ruptured and infected) HC was identified in the left lower lobe, measuring 12 × 12 × 11 cm, characterized by a thick, irregularly enhancing wall and a prominent air–fluid level with undulating internal membranes, consistent with the water-lily sign (Figure 2).
Therapeutic intervention
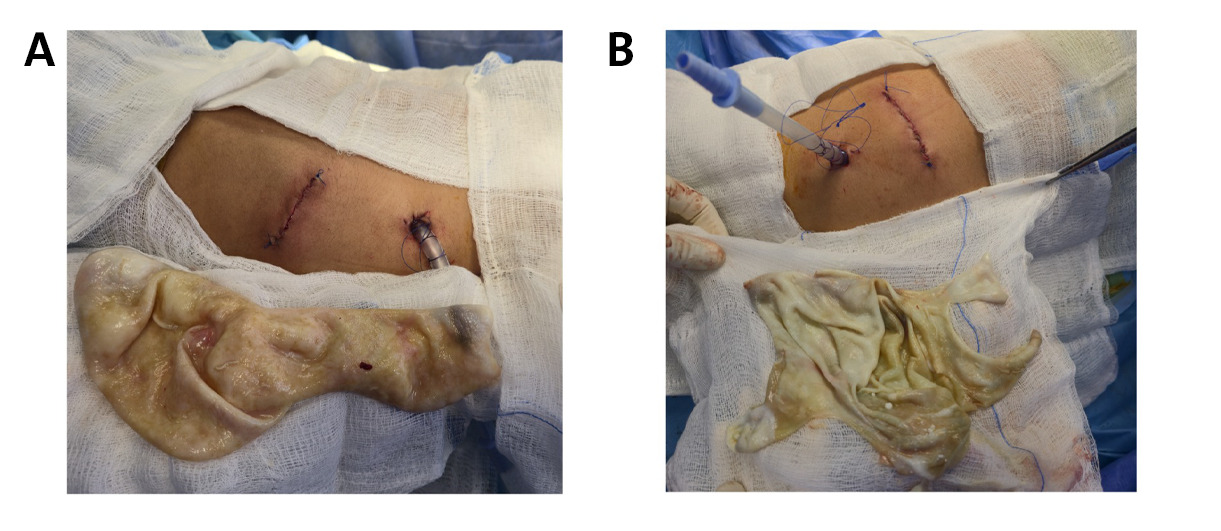
Under general anesthesia, the patient was placed in the left lateral decubitus position. Single-lumen endotracheal intubation was used with intermittent apnea as the patient did not tolerate single-lung ventilation. A bi-port VATS approach was employed. Controlled cyst drainage was performed, the germinal membrane was removed (Figure 3), and the cavity was irrigated with hypertonic saline (20% NaCl), followed by pericystectomy, closure of the bronchopleural fistulae, and capitonnage. Intercostal nerve cryoablation was performed from levels 3 to 11.
A chest tube was inserted, and the patient was repositioned to the right lateral decubitus position. The same procedure was repeated; however, dense pleural adhesions with pleural thickening and a foul odor were encountered. Therefore, extensive irrigation with hypertonic saline (20% NaCl) was performed, and bronchopleural fistulae were closed without capitonnage. Intraoperative pleural fluid culture revealed growth of Pseudomonas aeruginosa.
Follow-up
Postoperatively, the patient was empirically started on oral Amoxicillin–clavulanate (1 g twice daily for 3 days) and albendazole (400 mg twice daily). Albendazole therapy was continued (400 mg twice daily for 3 months). The postoperative course was uneventful, and she has remained well during 6 months of follow-up. She continues to be followed up on regularly.
Discussion
Uncomplicated pulmonary HCs are often asymptomatic and are frequently discovered incidentally on imaging. Their slow growth may contribute to delayed clinical presentation. When symptoms occur, pulmonary hydatid disease most commonly presents with cough, chest pain, fever, and hemoptysis [8]. For the present report, twelve cases of pulmonary hydatid cysts were reviewed as part of a brief literature review (Table 1). Cough was the most frequently reported symptom, occurring in all cases, followed by dyspnea and fever, both in 6 cases [1,2,9-15]. In the present case, the patient presented with chest discomfort, a productive cough, and dyspnea on exertion. Pulmonary HCs can develop in any lobe; however, they most frequently affect the right lung, particularly the lower lobes. Approximately 60% of cases are reported in the right lower lobe [4].
|
Author, year [citation] |
Age/Sex |
Residence/ Contacts with dogs or cattle |
Presentation |
Location/Size (cm) |
Management |
Complications |
Postoperative Management |
Outcome |
|
Anari et al., 2023 [1] |
14/M |
NR/NR |
Abdominal pain, cough, nausea, and vomiting |
Bilateral/ Gigantic (unspecified) |
Bilateral anterolateral mini-thoracotomy |
None |
Albendazole |
Uneventful recovery |
|
Mayyaleh et al., 2025 [9] |
5/F |
Urban/No contact |
Left-sided flank pain, anorexia, hypoactivity, dyspnea on exertion, productive cough & fever |
Left lower lobe/ 9x8.5x11 |
Lateral thoracotomy and VATS |
None |
Albendazole (130 mg) for 30 days |
Uneventful recovery |
|
Aghajanzadeh et al., 2012 [10] |
20/F |
NR/NR |
Right upper quadrant pain, right-sided chest pain, persistent cough, and a low-grade fever |
Bilateral/Giant (unspecified) |
Bilateral antero-lateral thoracotomies and phrenotomy |
None |
Albendazole for 90 days |
Uneventful recovery |
|
Alpay et al., 2012 [11] |
16/M |
NR/NR |
Fever, shortness of breath, and recurrent attacks of cough. |
Left lower lobe/ 5x4.5 |
VATS |
None |
None |
Uneventful recovery |
|
40/F |
NR/NR |
Recurrent attacks of cough |
Left lower lobe/5x5 |
VATS |
None |
None |
Uneventful recovery |
|
|
30/M |
NR/NR |
Recurrent attacks of cough |
Left lower lobe/4x4 |
VATS |
None |
None |
Uneventful recovery |
|
|
28/M |
NR/NR |
Recurrent attacks of cough and shortness of breath |
Left lower lobe/4x4 |
VATS |
None |
None |
Uneventful recovery |
|
|
Abubaker et al., 2026 [8] |
19/F |
Rural/None |
Persistent dry cough, shortness of breath, and left flank pain |
Bilateral L:15x11 R:10x6.8 |
Bronchoscopy and uVATS |
Right pneumothorax |
Albendazole for 6 months and a pigtail catheter for pneumothorax |
Uneventful recovery |
|
Ganguly et al., 2012 [12] |
8/F |
Rural/None |
Low-grade fever, occasional abdominal pain, and a non-productive cough |
Bilateral, R:7.4x6.7 L:8.5x6.4 |
Oral Albendazole, Postero-lateral thoracotomy |
None |
Albendazole |
Uneventful recovery |
|
Sabr et al., 2024 [13] |
15/M |
Rural/Yes |
Dyspnea and a persistent cough |
Bilateral R:16x14 L:14x12 |
VATS |
None |
Albendazole for 6 months |
Uneventful recovery |
|
Arega et al., 2022 [14] |
3/M |
NR/Yes |
Progressive dry cough, shortness of breath, and low-grade intermittent fever |
Bilateral R:9x7 L:8x7 |
Posterolateral thoracotomy and cystectomy |
None |
Albendazole |
Uneventful recovery |
|
Alawadhi et al., 2025 [15] |
42/M |
Rural/None |
Fever, chills, productive cough, and malaise |
Right lower lobe/ 4x2.9 |
Conservative |
Secondary bacterial infection and pleural effusion |
N/A |
Improvement of symptoms |
|
M: Male, F: Female, NR: Not reported, CM: Centimeter, VATS: Video-assisted thoracoscopic surgery, N/A: Not applicable |
|
|||||||
Imaging plays a central role in the diagnosis of hydatid disease. Chest X-rays and CT scans are particularly useful for identifying characteristic cystic lung lesions [13]. In uncomplicated pulmonary hydatid disease, the typical chest radiographic appearance consists of single or multiple well-defined, round masses with smooth borders and homogeneous density [9]. In the present case, chest radiography demonstrated a well-defined opacity in the right upper zone and a cavitary lesion in the left lower zone. The radiographic crescent sign, often linked to HCs, can also be observed in other conditions, including aspergilloma, cavitating malignancies, blood clots, and Rasmussen aneurysm [9]. The CT appearance of HCs can be variable and may occasionally mimic solid tumors due to associated inflammatory changes [9]. In cases such as the present one, particularly when the cyst is ruptured or infected, imaging may reveal a thick, irregularly enhancing wall and a prominent air–fluid level with undulating internal membranes, producing the characteristic water-lily sign.
Management of bilateral pulmonary hydatidosis remains controversial. It can be performed either as a one-stage procedure or as a two-stage approach, typically spaced 4–5 weeks apart, beginning with the uncomplicated cyst [8]. Due to intolerance of single-lung ventilation, this case underwent a single-stage surgery, as some authors advocate a single-stage procedure, citing advantages such as reduced morbidity, shorter hospitalization, and lower overall costs [8]. VATS has been employed as a minimally invasive alternative to reduce the risks associated with open surgery. However, its use is limited to select cases due to concerns about postoperative complications, including cyst rupture, spillage of cystic contents, and the management challenges associated with bronchial fistulas [5]. Hybrid interventions have also been utilized, though open surgery remains more common [4].
Among the reviewed cases, open surgical approaches were employed in four patients, all of whom experienced uneventful recoveries [1,10,12,14]. VATS was utilized in seven cases, with no reported complications, suggesting favorable outcomes in carefully selected patients [8,9,11,13]. These findings highlight that both open surgery and VATS can achieve good outcomes when appropriately indicated, although VATS may offer advantages in terms of reduced invasiveness. In contrast, conservative approaches may carry a greater risk of complications depending on case complexity and selection. In the present case, a single-stage VATS approach was adopted, given its association with lower morbidity, shorter hospital stays, and reduced overall cost [4].
A key controversy in the surgical management of pulmonary HCs is whether capitonnage should be performed following cystotomy. Traditionally, it has been recommended to obliterate the residual cavity; however, some authors suggest it may be unnecessary, emphasizing that meticulous closure of bronchial openings alone can allow adequate re-expansion and healing of the lung parenchyma [4]. In the present case, capitonnage was performed on the right side but omitted on the left side, where the infected, thickened pericyst precluded safe suturing. The patient had an uneventful recovery.
Adjunctive medical therapy with anthelmintic agents, such as albendazole, complements surgical management by reducing the risk of recurrence and targeting residual cystic elements [13]. In seven of the reviewed cases, albendazole was administered as postoperative therapy, and all patients had uneventful recoveries. The only exception was a case managed without surgical intervention, which reported only symptomatic improvement, not full recovery [15]. This pattern suggests that albendazole might be most effective as an adjunct to surgery rather than as a standalone treatment, supporting its role in reducing recurrence.
This report has some limitations. First, serological confirmation was not obtained, which would have provided additional diagnostic support, although serology is not always sensitive in pulmonary hydatid disease. Second, the follow-up period was relatively short, which limits the assessment of long-term outcomes and recurrence.
Conclusion
Single-session bilateral VATS may be a feasible therapeutic approach for giant pulmonary hydatid cysts, even when complicated cysts are present.
Declarations
Conflicts of interest: The authors have no conflicts of interest to disclose.
Ethical approval: Not applicable.
Consent for participation: Not applicable.
Consent for publication: Written informed consent for publication was obtained from the parents.
Funding: The present study received no financial support.
Acknowledgments: None to be declared.
Authors' contributions: FHK, AKH, and MMA: Major contributions to the study's conception and design, literature review, and manuscript drafting. HKA, AMM, and FHF: Contribution to the literature search, data collection, and manuscript preparation. HMH, HAA, SSA, KTS, and DOA: Critically revision of the manuscript and assisting in the preparation of the tables and figures. All authors have read and approved the final manuscript.
Use of AI: ChatGPT-5.3 was used to assist with language refinement and improve the overall clarity of the manuscript. All content was thoroughly reviewed and approved by the authors, who bear full responsibility for the final version.
Data availability statement: Not applicable.
References
- Anari S, Goli R, Faraji N, Rahimi K, Babamiri B, Zare F. Surgical excision for gigantic bilateral pulmonary hydatid cyst in a 14-year-old adolescent: a case report study. International Journal of Surgery Case Reports. 2023;109:108548. doi:10.1016/j.ijscr.2023.108548
- Mohammed TO, Ezzat SL, Abdullah HS, Qadir SJ, Hamad AK, Faraj SA, et al. Echinococcus granulosus in Environmental Samples: A Cross-Sectional Molecular Study. Barw Medical Journal. 2025;3(4):9-14. doi:10.58742/bmj.vi.200
- Aydin Y, Ulas AB, Kasali K, Eren S, Dostbil A, Eroglu A. Treatment of pulmonary hydatid cysts: a single-centre analysis of 872 cases. European Journal of Cardio-Thoracic Surgery. 2025;67(4):ezaf114. doi:10.1093/ejcts/ezaf114
- Kakamad FH. Thoracoscopic capitonnage for pulmonary hydatid cysts: the predictors of prolonged air leak. Frontiers in Surgery. 2025;12:1664976. doi:10.3389/fsurg.2025.1664976
- Abbas N, Zaher Addeen S, Abbas F, Al Saadi T, Hanafi I, Alkhatib M et al. Video-assisted Thoracoscopic Surgery (VATS) with mini-thoracotomy for the management of pulmonary hydatid cysts. Journal of Cardiothoracic Surgery. 2018;13(1):35.
- Prasad S, Nassar M, Azzam AY, García-Muro-San José F, Jamee M, Sliman RK, et al. CaReL Guidelines: A Consensus-Based Guideline on Case Reports and Literature Review (CaReL). Barw Med J. 2024;2(2):13-19. doi:10.58742/bmj.v2i2.89
- Kakamad FH, Mohammed SH, Abdalla BA, Hussein DA, Hammood ZD, Kakamad SH, et al. Non-Recommended Publishing Lists: Strategies for Detecting Deceitful Journals. Barw Medical Journal. 2026;4(1):13-21. doi:10.58742/bmj.v4i1.227
- Abubaker AN, Hroub SI, Dawada AN, Diab LK, Salah Q, Asbeh YA. An atypical case of bilateral pulmonary hydatid cyst with endo-rupture managed with two-stages uniportal video-assisted thoracoscopic surgery in Palestine: case report. International Journal of Surgery Case Reports. 2026;138(3):1017-21. doi:10.1097/RC9.0000000000000299
- Mayyaleh HA, Abu-Radwan B, Jadallah I, Saleh M, Fasfoos A, Asbeh YA. When size matters: Managing a giant pulmonary hydatid cyst in a pediatric patient: Case report. Medicine. 2025;104(37):e44212. doi:10.1097/md.0000000000044212
- Aghajanzadeh M, Aghajanzadeh G, Ebrahimi H, Jahromi SK, Maafi AA, Massahnia S. One stage operation for five giant hydatid cysts of both lungs and liver in a 20-year-old female. Tanaffos. 2012;11(3):52.
- Alpay L, Lacin T, Atinkaya C, Kıral H, Demir M, Baysungur V et al. Video-assisted thoracoscopic removal of pulmonary hydatid cysts. European journal of cardio-thoracic surgery. 2012;42(6):971-5. doi:10.1093/ejcts/ezs338
- Ganguly S, Samanta M, Chatterjee S. Bilateral giant-sized symmetrical pulmonary hydatid cysts in an 8-year-old girl. Paediatrics and international child health. 2012;32(3):180-2. doi:10.1179/2046905511Y.0000000010
- Sabr WN, Hattam AS, Hasan KM, Kareem HO, Ahmed HK, Kakamad SH et al. Bilateral Giant Hydatid Pulmonary Cysts in a Pediatric Patient: A Rare Case Report. Barw Medical Journal. 2024;2(2):63-67. doi:10.58742/beb68v43
- Arega G, Kebede RA, Woldeselassie HG, Lingerh T, Yayeh T. Bilateral large pulmonary hydatid cyst: a rare presentation in a young child from Ethiopia. Pediatric Health, Medicine and Therapeutics. 2022:279-82. doi:10.2147/PHMT.S374091
- Alawadhi KY, Alkhoori SA, Alshamsi SA, Baroud S, Awawdeh R, Almadi R et al. Isolated Ruptured Pulmonary Hydatid Cyst Mimicking Community-Acquired Pneumonia. Cureus. 2025;17(10). doi:10.7759/cureus.95612

Copyright (c) 2026 The Author(s)

This work is licensed under a Creative Commons Attribution 4.0 International License.