Coexisting Granulomatous Mastitis and Breast Cancer: A Systematic Review

Abstract
Introduction: Granulomatous mastitis (GM) is a rare inflammatory breast disease that mimics carcinoma. GM can coexist with breast cancer (BC), though the relationship remains unclear. This systematic review aims to examine the coexistence of GM and BC, focusing on the clinicopathological features of synchronous and metachronous cases.
Methods: A systematic search of PubMed/MEDLINE and Google Scholar, up to the 30th November 2025, identified studies reporting individual patient-level data. Inclusion criteria were: (1) patients diagnosed with both BC and GM (concurrently or sequentially); (2) histopathological or imaging confirmation of both conditions. Exclusion criteria were: (1) animal studies; (2) conference abstracts; (3) non-recommended journal publications; and (4) non-English papers. Descriptive statistics were used to summarize categorical variables as frequencies and percentages, and continuous variables as means or medians with ranges.
Results: Nineteen studies (23 female patients; median age of 42 years) were included. Most of the cases were premenopausal 17 (74.0%). Synchronous coexistence occurred in 15 (65.2%), with ipsilateral involvement in 11 (73.3%) of these. Granulomatous mastitis preceded BC in 6 (26.1%) (median interval 3 years), and BC preceded GM in 2 (8.7%). Core needle biopsy diagnosed GM in 9 (39.1%) and BC in 14 (60.9%); excisional biopsy was required in 7 (30.4%) of GM cases. Breast cancer treatment included mastectomy in 11 (47.8%) and breast-conserving surgery in 9 (39.1%). Follow-up ranged from 2–53 months.
Conclusion: Granulomatous mastitis and BC can coexist, with GM potentially masking malignancy. Clinicians should maintain a low threshold for repeat biopsy in refractory cases.
Introduction
Granulomatous mastitis (GM) is a rare, chronic inflammatory breast disease, first described in 1972 as a lesion mimicking carcinoma [1,2]. It is characterized by non-caseating granulomatous inflammation centered on breast lobules, typically affecting women of childbearing age, often within five years of their last childbirth [3,4]. The incidence of idiopathic GM is estimated at 2.4 per 100,000 women aged 20-40 years, with higher rates among Asian, Hispanic, and Arab populations [5]. Although the exact etiology remains unclear, proposed mechanisms include autoimmune processes, hormonal imbalances, oral contraceptive use, hyperprolactinemia, pregnancy and lactation, alpha-1 antitrypsin deficiency, and infectious agents [6,7]. While GM is generally benign, several reports have documented its occurrence alongside breast carcinoma. The coexistence of GM and breast cancer (BC) presents a rare but clinically significant diagnostic and therapeutic challenge [7]. The literature contains case reports and small series of patients with concurrent or metachronous GM and BC, encompassing invasive ductal carcinoma (IDC), ductal carcinoma in situ (DCIS), and lobular carcinoma in situ (LCIS) [8,9]. The pathophysiological relationship between GM and BC is not fully understood. Two main hypotheses have been proposed. First, the granulomatous response may represent a secondary "sarcoid-like reaction" to breast carcinoma first described in 1911, reflecting immunological hypersensitivity to tumor-derived antigens [7,10]. Second, chronic inflammation from GM may predispose to dysplasia and subsequent malignant transformation [7,10]. This systematic review aims to examine the coexistence of GM and breast carcinoma, focusing on the clinicopathological features of synchronous and metachronous cases.
Methods
Study design
This review followed Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines [11].
Information sources and search strategy
A systematic literature search was conducted in PubMed/MEDLINE and Google Scholar for published studies up to 30th of November 2025. The following medical keywords and search terms were used for Google Scholar: (cancer OR cancers OR cancerous OR carcinoma OR carcinomas OR neoplasm OR neoplasms OR malignancy OR malignancies OR malignant OR metastasis OR tumor OR tumors) AND ("granulomatous mastitis" OR GM). And these keywords were used in PubMed/MEDLINE: ("granulomatous mastitis"[tiab] OR GM [tiab] OR "Granulomatous Mastitis"[Mesh]) AND (cancer[tiab] OR cancers[tiab] OR carcinoma[tiab] OR carcinomas[tiab] OR neoplasm[tiab] OR neoplasms[tiab] OR malignancy[tiab] OR malignancies[tiab] OR malignant[tiab] OR metastasis[tiab] OR tumor[tiab] OR tumors[tiab] OR "Breast Neoplasms"[Mesh]).
Inclusion Criteria
Studies were included if they met the following criteria: 1) Studies reporting individual patient-level data, 2) patients diagnosed with both GM and BC, either concurrently or sequentially, 3) the diagnosis of both BC and GM was confirmed by diagnostic imaging, surgical findings, or histopathological examination. All included studies underwent eligibility verification [12].
Exclusion Criteria
Exclusion criteria included all of the following: 1) Studies with no human subjects, 2) studies that were published in the form of conference abstracts, 3) studies published in non-recommended journals, and 4) non-English papers.
Data extraction
The extracted data included the following variables: The first author's name, year of publication, and country of study. Patient demographic and reproductive characteristics included age, parity, menopausal status, lactation history, oral contraceptive use, and smoking status. Clinical presentation data included the chief complaint, duration of symptoms before diagnosis, side and quadrant of the affected breast, and family history of BC. Regarding the relationship between GM and BC, the laterality of each pathology and the chronological sequence of the two diagnoses were recorded. Diagnostic data included the sampling and diagnosis method, type of GM, and imaging findings on mammography, ultrasound, and magnetic resonance imaging (MRI), along with the assigned Breast Imaging-Reporting and Data System (BI-RADS) category. Breast cancer-specific variables comprised the type and grade of cancer, hormone receptor status such as estrogen receptor (ER), progesterone receptor (PR), and human epidermal growth factor receptor 2 (HER2), cancer stage, and metastasis status. Finally, management data included the treatment approaches applied for both GM and BC, and the follow-up duration. Granulomatous Mastitis and BC were classified as synchronous when both were diagnosed concurrently or within 6 months of one another, and as metachronous when the interval between the two diagnoses exceeded 6 months [13].
Statistical Analysis
Descriptive statistics were used to summarize categorical variables as frequencies and percentages. Continuous variables (e.g., age, follow-up duration) were summarized as means with ranges or medians with ranges, as appropriate. All analyses were conducted using Microsoft Excel (version 16.0).
Results
Study selection
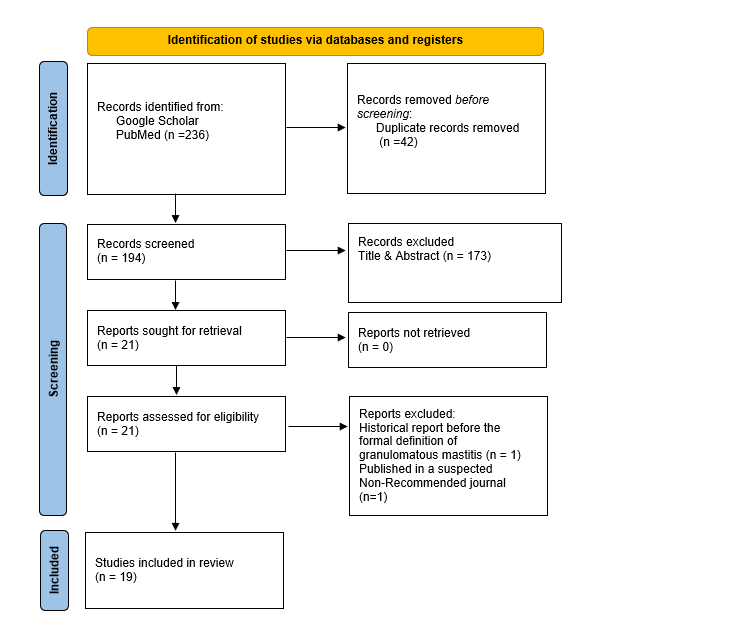
A total of 236 records were identified from PubMed/MEDLINE and Google Scholar. After removing 42 duplicates, 194 records were screened. Of these, 173 were excluded based on title and abstract review, leaving 21 reports to be sought for retrieval, all of which were successfully retrieved. Following eligibility assessment, 2 reports were excluded (one as it was a historical report predating the formal definition of GM, and the other one due to publication in a non-recommended journal). Ultimately, 19 studies were included in the final review (Figure 1).
Characteristics of the included studies
A comprehensive literature search yielded a total of 23 eligible cases from 19 published reports [2,4-10,14-24] documenting the coexistence of GM and BC. These cases were derived from case reports and case series published between 2012 and 2025. The included cases originated from multiple countries; most commonly from Iran (7, 30.4%) and China (5, 21.7%), followed by Iraq and Turkey (2, 8.7%), with single cases reported from Brazil, Chile, Japan, Australia, Malaysia, Tunisia, and Pakistan (Tables 1 & 2).
|
Author (year) [ref] |
N |
Country |
Age (years) |
Presentation |
Duration of Symptoms |
Parity |
Menopausal |
Lactation |
OCP |
Smoking |
FH of BC |
|
Salih et al., 2025 [2] |
1 |
Iraq |
36 |
Breast pain |
2w |
3 |
Pre |
4y, currently nursing |
No |
Passive |
No |
|
Freitas et al., 2020 [20] |
1 |
Brazil |
42 |
Breast nodule enlargement |
NA |
2 |
Pre |
5y |
No |
NA |
No |
|
Zavieh et al., 2024 [8]
|
3 |
Iran |
42 |
Breast Pain and lump |
NA |
2 |
Pre |
48m, 20y ago |
Yes |
NA |
No |
|
46 |
Mass |
NA |
2 |
Pre |
9y before GM |
No |
NA |
No |
|||
|
41 |
Mass |
NA |
NA |
Pre |
NA |
No |
NA |
No |
|||
|
Zhu et al., 2024 [18]
|
3 |
China |
51 |
Hard mass |
1d |
NA |
Post |
NA |
NA |
NA |
NA |
|
50 |
Recurrent mass |
NA |
NA |
Peri |
NA |
NA |
NA |
NA |
|||
|
45 |
Lump with redness, heat, pain, nipple retraction and discharge |
2m |
NA |
Peri |
NA |
NA |
NA |
NA |
|||
|
Oddó et al., 2019 [6] |
1 |
Chile |
44 |
Pain and swelling |
2w |
NA |
NA |
NA |
NA |
Former |
No |
|
Tavakol et al., 2022 [9] |
1 |
Iran |
35 |
Pain & mass |
1m |
2 |
Pre |
NA |
No |
NA |
No |
|
Yoshida et al., 2023 [4] |
1 |
Japan |
34 |
Mass & redness |
NA |
NA |
Pre |
NA |
NA |
NA |
No |
|
Zangouri et al., 2022 [22] |
1 |
Iran |
38 |
Mass |
NA |
NA |
Pre |
28m |
NA |
NA |
NA |
|
Çalış and Kilitçi, 2018 [19] |
1 |
Turkey |
77 |
Pain & swelling |
NA |
NA |
Post |
NA |
NA |
NA |
NA |
|
Xie et al., 2022 [23] |
1 |
China |
39 |
Enlarging mass, pain, redness |
NA |
1 |
Pre |
NA |
NA |
NA |
No |
|
Evans et al., 2021 [17] |
1 |
Australia |
39 |
Mass increasing in size & tenderness |
NA |
2 |
Pre |
NA |
NA |
NA |
No |
|
Salih et al., 2023 [16] |
1 |
Iraq |
30 |
Pain |
7d |
3 |
Pre |
6m, 3y ago |
No |
No |
Yes |
|
Mazlan et al., 2012 [24] |
1 |
Malaysia |
34 |
Progressive loss of vision in the left eye |
NA |
NA |
Pre |
NA |
No |
No |
No |
|
Chen et al., 2025 [21] |
1 |
China |
31 |
Mass, pain |
NA |
NA |
Pre |
Currently Lactating, 4y3m |
NA |
NA |
NA |
|
AkbariRad et al., 2025 [7] |
1 |
Iran |
46 |
Stiffness |
NA |
3 |
Pre |
NA |
No |
NA |
Yes |
|
Limaiem et al., 2013 [10] |
1 |
Tunisia |
77 |
Pain |
6m |
NA |
Post |
NA |
No |
NA |
NA |
|
Özşen et al., 2018 [14] |
1 |
Turkey |
35 |
Swelling |
8m* |
0 |
Pre |
NA |
NA |
NA |
NA |
|
Mahmood et al., 2025 [5] |
1 |
Pakistan |
45 |
Painful breast swelling |
NA |
7 |
Pre |
2 y for each 7 children |
NA |
No |
No |
|
Kaviani et al., 2017 [15] |
1 |
Iran |
48 |
large palpable masses and nipple retraction
|
4m |
NA |
Pre |
None |
Yes |
NA |
No |
|
Abbreviations. Ref: reference; GM: granulomatous mastitis Pre: premenopausal; Post: postmenopausal; Peri: perimenopausal; FH: family history; BC: breast cancer; OCP: oral contraceptive pills; NA: not available; D: days; W: weeks; M: months; Y: years. *First experienced swelling in her right breast in March 2017, the case report was formally received for publication on November 26, 2017 |
|||||||||||
|
Variable |
N |
% |
|
Country Iran China Iraq Turkey Other countries |
7 5 2 2 7 |
30.4 21.7 8.7 8.7 30.4 |
|
Age (years) 30-39 40-49 50-59 ≥60 |
10 9 2 2 |
43.5 39.1 8.7 8.7 |
|
Menopausal status Premenopausal Perimenopausal Postmenopausal N/A |
17 2 3 1 |
74.0 8.7 13.0 4.3 |
|
Parity Nulliparous (0) Primiparous (1) Multiparous (2-3) Grand multiparous (≥7) N/A |
1 1 8 1 12 |
4.3 4.3 34.8 4.3 52.2 |
|
Lactation History Currently lactating Previous lactation No lactation history N/A |
2 6 1 14 |
8.7 26.1 4.3 60.9 |
|
Risk factors |
||
|
OCP use Yes No N/A |
2 9 12 |
8.7 39.1 52.2 |
|
Smoking history Former Passive No N/A |
1 1 3 18 |
4.3 4.3 13.0 78.3 |
|
Family history of BC Yes No N/A |
2 13 8 |
8.7 56.5 34.8 |
|
Granulomatous Mastitis Characteristics |
||
|
Side Left breast Right breast Bilateral |
14 8 1 |
60.9 34.8 4.3 |
|
Type Idiopathic GM Non-idiopathic GM |
20 3 |
87.0 13.0 |
|
Breast cancer characteristics |
||
|
Laterality Ipsilateral to GM Contralateral to GM Bilateral GM |
16 6 1 |
69.6 26.1 4.3 |
|
Type of carcinoma IDC DCIS Mixed (IDC+DCIS) LCIS |
13 7 2 1 |
56.5 30.4 8.7 4.3 |
|
Cancer grade High-grade Intermediate-grade Low-grade N/A |
12 3 2 6 |
52.2 13.0 8.7 26.1 |
|
Molecular subtype |
||
|
ER Positive Negative N/A |
14 5 4 |
60.9 21.7 17.4 |
|
PR Positive Negative N/A |
10 7 6 |
43.5 30.4 26.1 |
|
HER2 Positive Negative N/A |
7 9 7 |
30.4 39.1 30.4 |
|
Triple-negative |
3 |
13.0 |
|
Cancer stage Stage 0 Stage 1 Stage 2 Stage 3 Stage 4 N/A |
8 1 9 2 1 2 |
34.8 4.3 39.1 8.7 4.3 8.7 |
|
Temporal Relationship Synchronous Metachronous GM before BC BC before GM |
15 8 6 2 |
65.2 34.8 26.1 8.7 |
|
Diagnosis Method |
||
|
GM diagnosis Core needle biopsy only Excisional / Incisional Biopsy (EB/IB) Only Mixed methods N/A |
9 7 5 2 |
39.1 30.4 21.7 8.7 |
|
Breast Cancer Diagnosis Core needle biopsy only Excisional / Incisional Biopsy (EB/IB) Only Mixed methods N/A |
14 5 2 2* |
60.9 21.7 8.7 8.7 |
|
Treatment of Granulomatous Mastitis Surgical intervention only Conservative management only Mixed |
3 8 12 |
13.0 34.8 52.2 |
|
Treatment of Breast Cancer Mastectomy Breast-conserving surgery Hormone therapy Radiotherapy Neoadjuvant chemotherapy Adjuvant chemotherapy |
11 9 9 8 7 6 |
47.8 39.1 39.1 34.8 30.4 26.1 |
|
Abbreviations. N/A: not available; GM: granulomatous mastitis; BC: breast cancer; OCP: oral contraceptive pills; IDC: invasive ductal carcinoma; DCIS: ductal carcinoma in situ; LCIS: lobular carcinoma in situ; ER: estrogen receptor; PR: progesterone receptor; HER2: human epidermal growth factor receptor 2. *Chen et al. (2025) was classified as N/A because the biopsy technique was not explicitly reported. |
||
Participants
A total of 23 female patients with coexisting GM and BC were analyzed. The median age was 42 years (range 30–77 years). The majority were premenopausal (17, 74.0%), followed by postmenopausal (3, 13.0%), and perimenopausal (2, 8.7%); menopausal status was not applicable in 1 (4.3%). Parity data were available for 11 patients: 1 (9.1%) was nulliparous, 1 (9.1%) was primiparous, 8 (72.7%) were multiparous with 2–3 children, and 1 (9.1%) was grand multiparous with 7 children. Lactation history was documented in 9 patients (39.1%): 2 (22.2%) were currently lactating at presentation, 6 (66.7%) had previous lactation ranging from 6 months to 9 years, and 1 (11.1%) had no lactation history. Risk factors were incompletely reported. Oral contraceptive pill use was explicitly denied in 9 (39.1%) and confirmed in 2 (8.7%) (Tables 1 & 2).
Main Findings
Imaging findings were nonspecific and overlapping between GM and BC. Mammography was performed in 13 (56.5%) of cases, commonly showing asymmetric density, focal opacity, calcifications, or mass lesions. Ultrasound was used in 22 (95.7%) cases, frequently demonstrating irregular hypoechoic areas in 12 (54.5%), heterogeneous echogenicity in 4 (18.2%), skin thickening in 5 (22.7%), ductal dilatation in 3 (13.6%), and occasionally fluid collections or abscesses in 3 (13.6%). Magnetic resonance imaging was performed in 11 (47.8%) cases, revealing non-mass enhancement in 3 (27.3%), rim enhancement in 1 (9.1%), ductal dilatation in 3 (27.3%), and washout kinetic curves suggestive of malignancy in 4 (36.4%). BI-RADS categories ranged from 2 to 5. Among the 9 cases (39.1%) with a documented BI-RADS category, all 9 (100%) had at least one lesion categorized as BI-RADS 4 or 5, indicating high suspicion for malignancy. In 3 cases (13.0%), GM-associated inflammation initially obscured malignant features on imaging, and only after treatment of GM did the underlying cancer become more apparent (Table 3).
|
Author (year) [ref] |
MMG |
US |
MRI |
BI-RADS |
|
Salih et al., 2025 [2] |
N/A |
Heterogeneous area with fluid echogenicity and moderate surrounding edema; localized skin thickening and contour distortion at 2 o'clock (64x27 mm) |
Heterogeneous non-mass-like enhancement and a small 18-mm central mass; bilateral enlarged axillary lymph nodes |
N/A |
|
Freitas et al., 2020 [20] |
N/A |
BI-RADS 4c lesion initially; follow-up showed a residual nodule and a new palpable area |
A 3-cm irregular nodule with a Type 3 kinetic curve and a 2.4-cm axillary lymph node |
4C(US) |
|
Zavieh et al., 2024 [8]
|
Focal density in the central outer part of the breast |
50x29x22 mm mass-like lesion with undefined borders and dilated ducts containing debris and extending toward the nipple. |
N/A |
4 (US) |
|
N/A |
Hypoechoic irregular spiculated mass with indistinct margins |
N/A |
N/A |
|
|
N/A |
22x20 mm irregular hypoechoic mass |
N/A |
5 (US) |
|
|
Zhu et al., 2024 [18]
|
N/A |
Glandular edema and dilated ducts |
Posterior edema of the glandular layer with ductal dilatation |
N/A |
|
enlarged ducts with dense calcification resembling gravel in the ducts |
Local glandular hypertrophy with multiple internal hypoechoic nodules |
Abnormal mass shadowing and ductal dilatation |
4A (US) |
|
|
N/A |
Multiple fluid-filled dark areas |
N/A |
N/A |
|
|
Oddó et al., 2019 [6] |
Diffuse dense breast with focal areas of higher density; no microcalcifications |
Cutaneous thickening, increased echogenicity of subcutaneous tissue, and multiple collections |
N/A |
N/A |
|
Tavakol et al., 2022 [9] |
Large mass (150 mm) in the lateral part of the right breast; no distortion |
Right: Diffuse heterogeneous ill-defined area with internal microcalcification and skin thickening. Left: well-defined hypoechoic mass |
R: Asymmetrical parenchymal thickening, multiple rim-enhanced masses (14–35 mm), and extensive NME (140x80x60 mm) with a Type 3 curve |
4B (US) / 4C (MRI) |
|
Yoshida et al., 2023 [4] |
N/A |
Irregular hypoechoic area measuring > 4 cm |
Widespread T2-weighted high-signal lesion with a fast washout pattern and pre-spectral edema |
Initial:4B (MRI) Follow-up: 4A (MRI) |
|
Zangouri et al., 2022 [22] |
Well-defined high-density mass |
Irregular hypoechoic mass with tubular extensions |
N/A |
N/A |
|
Çalış and Kilitçi, 2018 [19] |
Amorphous mass and focal asymmetric opacity with calcifications |
Fibroglandular tissue increases with no distinctive borders; inflammatory appearance with right axillary non-reactive lymphadenopathy |
N/A |
N/A |
|
Xie et al., 2022 [23] |
N/A |
Diffusely distributed irregular hypoechoic lesions; skin thickening and increased echogenicity in subcutaneous tissue |
N/A |
4 (US) |
|
Evans et al., 2021 [17] |
Left (GM): Asymmetric density with hyperemia; Right (BC): Clusters of pleomorphic microcalcifications |
Left (GM): 60-mm irregularity (no collection); Right (BC): irregular lesions measuring 16x11x11 mm and 9x10x7 mm |
60mm resectable area |
N/A |
|
Salih et al., 2023 [16] |
Left: Operative bed deformity, skin thickening, and two rounded scattered faint micro-calcifications below the scar. Right: Solitary benign-looking calcification. |
Full-length ectatic duct from nipple root to 5–7 o'clock; heterogeneous internal echo and mild surrounding edema |
Clumped focal non-mass-like enhancement (20x6 mm) within an ectatic duct; surgical bed showed additional heterogeneous NME (19x13 mm) |
2 (MMG) / 4 (MRI) |
|
Mazlan et al., 2012 [24] |
Extensive scarring |
Extensive fibrous scarring noted during follow-up |
Breast scarring suspicious for malignancy; orbital apex tumor compressing the optic nerve. |
N/A |
|
Chen et al., 2025 [21] |
Heterogeneous density with uneven distribution; no definite mass |
Patchy hypoechoic area (8.3 × 1.0 cm) beneath the nipple with irregular shape, clear boundaries, partial ductal distribution, and uneven internal echoes. Color Doppler showed abundant peripheral strip-like blood flow. CEUS revealed rapid, high enhancement with small non-enhanced foci (~1.1 × 0.2 cm). Follow-up imaging confirmed sinus tract formation connecting multiple hypoechoic areas to the skin |
Multiple hyperintense T2 signal lesions; post-contrast nodules and patchy enhancements in the lower quadrant with a washout-type curve |
N/A |
|
AkbariRad et al., 2025 [7] |
N/A |
An ill-defined mass (32x26 mm) in the central region of the right breast |
N/A |
N/A |
|
Limaiem et al., 2013 [10] |
A 2.2 x 2.4 cm stellate mass with uneven edges. |
NA |
N/A |
N/A |
|
Özşen et al., 2018 [14] |
NA |
Heterogeneous, irregularly limited hypoechoic area (3 cm from the subareolar zone), with a 34x9 mm fluid pocket at the 12 o'clock position. |
N/A |
N/A |
|
Mahmood et al., 2025 [5] |
Suspicious UOQ lesion |
Left (Initial): 25.7mm irregular hypoechoic mass + axillary thickening (IDC). Bilateral (Interval): Skin thickening, parenchymal fuzziness, and ductal dilatation with internal avascular echoes (IGM onset) |
N/A |
L:4 (MMG) R:2 (US) |
|
Kaviani et al., 2017 [15] |
Distortion and mass-like lesions within extremely dense breast tissue |
Right: Large hypoechoic mass with irregular borders and multiple echogenic foci; Left: Hypoechoic spiculated mass (30x50 mm). |
Post-chemo: a single mass (20x12 mm) in the left breast without satellite lesions. |
N/A |
|
Abbreviation. Ref: reference; MMG: mammography; US: ultrasonography; MRI: magnetic resonance imaging; BI-RADS: Breast Imaging Reporting and Data System; N/A: not available; IDC: invasive ductal carcinoma; IGM: idiopathic granulomatous mastitis; CEUS: contrast-enhanced ultrasound; NME: non-mass enhancement; UOQ: upper outer quadrant; L: left; R: right; GM: granulomatous mastitis; BC: breast cancer; chemo: chemotherapy |
||||
Synchronous coexistence of GM and BC occurred in 15 (65.2%) cases. Among these, the majority demonstrated ipsilateral involvement, with BC arising in the same breast as GM in 11 (73.3%) of synchronous cases. Contralateral GM relative to the cancer was observed in 3 (20.0%), while bilateral GM was observed in 1 (6.7%). The most common BC histologies in synchronous cases were DCIS alone, accounting for 6 (40.0%), and IDC alone in 6 (40.0%), followed by mixed IDC and DCIS in 2 (13.3%), and LCIS in 1 (6.7%). High-grade tumors were observed in 8 (53.3%) of synchronous cases, intermediate-grade in 2 (13.3%), low-grade in 2 (13.3%); grade was not reported in 3 (20.0%) (Tables 2 & 4).
|
Author (year) [ref] |
Side |
Quadrant |
Laterality (GM) |
Chronology (GM) |
Diagnosis method |
GM Type |
BC Type |
Grade |
ER |
PR |
HER2 |
AJCC |
|
Salih et al., 2025 [2] |
L |
UOQ |
Ipsilateral |
Synchronous |
GM&BC: CNB |
Idio |
IDC+DCIS |
High |
+ |
NA |
+ |
2A |
|
Freitas et al., 2020 [20] |
R |
UOQ |
Ipsilateral |
Synchronous (after BC during chemotherapy) |
GM&BC: CNB
|
Non-Idio |
IDC |
High |
+ |
+ |
- |
1A |
|
Zavieh et al., 2024 [8]
|
L |
Lateral |
Contralateral |
Metachronous (2 years after BC treatment) |
GM: CNB and IB; BC:N/A |
Idio |
IDC |
N/A |
+ |
+ |
+ |
2 |
|
R |
N/A |
Ipsilateral |
Metachronous (4 years before BC) |
GM: N/A; BC: CNB
|
Idio |
IDC |
N/A |
- |
- |
- |
N/A |
|
|
L |
N/A |
Contralateral |
Metachronous (13 years before BC) |
GM: N/A; BC: CNB |
Idio |
IDC |
N/A |
+ |
+ |
+ |
N/A |
|
|
Zhu et al., 2024 [18]
|
L |
LOQ+LIQ |
Ipsilateral |
Synchronous |
GM&BC: CNB |
Idio |
DCIS |
High |
- |
- |
- |
0 |
|
L |
Lateral |
Ipsilateral |
Synchronous |
GM&BC: EB |
Idio |
DCIS |
High |
- |
- |
+ |
0 |
|
|
L |
N/A |
Ipsilateral |
Synchronous |
GM: EB; BC: CNB
|
Non-Idio |
DCIS |
Low |
+ |
+ |
+ |
0 |
|
|
Oddó et al., 2019 [6] |
L |
UOQ + LOQ |
Ipsilateral |
Synchronous |
GM&BC: CNB and IB |
Idio |
DCIS |
Int |
+ |
+ |
N/A |
0 |
|
Tavakol et al., 2022 [9] |
R |
UOQ + Lateral |
Ipsilateral |
Synchronous |
GM&BC: CNB |
Idio |
LCIS |
N/A |
N/A |
N/A |
N/A |
0 |
|
Yoshida et al., 2023 [4] |
L |
LIQ |
Ipsilateral |
Synchronous |
GM: FNA and CNB; BC: EB |
Non-Idio |
DCIS |
Low |
+ |
+ |
N/A |
0 |
|
Zangouri et al., 2022 [22] |
L |
N/A |
Ipsilateral |
Metachronous (1 year before BC) |
GM&BC: CNB |
Idio |
IDC |
High |
N/A |
N/A |
N/A |
3A |
|
Çalış and Kilitçi, 2018 [19] |
R |
RA + UOQ |
Ipsilateral |
Synchronous |
GM&BC: CNB and EB |
Idio |
IDC+DCIS |
High |
- |
- |
+ |
2A |
|
Xie et al., 2022 [23] |
L |
Areolar + LOQ |
Ipsilateral |
Metachronous (BC masked by GM for 10 months)* |
GM: CNB; BC: EB
|
Idio |
IDC |
Int |
+ |
+ |
- |
2A |
|
Evans et al., 2021 [17] |
L |
UOQ |
Contra |
Synchronous |
GM: EB; BC: CNB |
Idio |
IDC |
High |
N/A |
+ |
- |
3A |
|
Salih et al., 2023 [16] |
L |
LIQ + LOQ |
Ipsilateral |
Metachronous (2 years before BC) |
GM&BC: EB
|
Idio |
DCIS |
High |
+ |
N/A |
N/A |
0 |
|
Mazlan et al., 2012 [24] |
R |
N/A |
Ipsilateral |
Metachronous (8 years before BC) |
GM: IB; BC: CNB |
Idio |
IDC |
High |
+ |
+ |
- |
4 |
|
Chen et al., 2025 [21] |
L |
LQ |
Contralateral |
Metachronous (3 years after radical mastectomy for BC) |
GM: EB; BC: Biopsy |
Idio |
IDC |
High |
- |
- |
- |
2B |
|
AkbariRad et al., 2025 [7] |
L |
Lateral |
Contralateral |
Synchronous |
GM&BC: CNB |
Idio |
IDC |
High |
+ |
- |
- |
2B** |
|
Limaiem et al., 2013 [10] |
R |
SA |
Ipsilateral |
Synchronous |
GM: EB; BC: CNB |
Idio |
IDC |
Int |
+ |
+ |
- |
2A |
|
Özşen et al., 2018 [14] |
R |
SA |
Ipsilateral |
Synchronous |
GM: CNB; BC: EB |
Idio |
DCIS |
N/A |
N/A |
N/A |
N/A |
0 |
|
Mahmood et al., 2025 [5] |
Bilat |
PA + RA |
Bilateral |
Synchronous (after the 2nd cycle of chemotherapy for BC) |
GM&BC: CNB
|
Idio |
IDC |
High |
+ |
- |
+ |
2B |
|
Kaviani et al., 2017 [15] |
R |
Central |
Contralateral |
Synchronous |
GM: CNB and IB; BC: CNB |
Idio |
IDC |
N/A |
+ |
N/A |
N/A |
2A |
|
Abbreviation. Ref: reference; L: left; R: right; UOQ: upper outer quadrant; LOQ: lower outer quadrant; LIQ: lower inner quadrant; LQ: lower quadrant; SA: subareolar; RA: retroareolar; PA: periareolar; GM: granulomatous mastitis; BC: breast cancer; CNB: core needle biopsy; EB: excisional biopsy; IB: incisional biopsy; FNA: fine needle aspiration; IDC: invasive ductal carcinoma; DCIS: ductal carcinoma in situ; LCIS: lobular carcinoma in situ; ER: estrogen receptor; PR: progesterone receptor; HER2: human epidermal growth factor receptor 2; N/A: not available; Idio: idiopathic; Non-Idio: non-idiopathic; Int: intermediate grade; AJCC: American Joint Committee on Cancer; +, positive; -, negative. * Although the clinical interval between diagnoses was 10 months, this case was classified as metachronous by standard criteria. The authors noted that the malignancy was likely present at the initial presentation. The intense inflammatory response and edema associated with GM provided a diagnostic masking effect, leading to a 10-month diagnostic lag. **The exact number of metastatic axillary lymph nodes was not reported in this case. However, the authors explicitly confirmed the presence of right axillary lymph node metastasis in their summary table. In the absence of quantitative nodal data, the case was classified as N1 based on categorical evidence of axillary nodal involvement. |
||||||||||||
In 6 (26.1%) cases, GM was diagnosed before BC, with intervals ranging from 10 months to 13 years (median approximately 3 years). All patients in this subgroup were premenopausal. The initial presentation of GM was typically a palpable breast mass, and all patients received treatment for GM including corticosteroids, methotrexate, or surgical drainage. Among these, 2 (33.3%) experienced recurrent GM before the cancer diagnosis. The subsequent BC was ipsilateral to the original GM in 5 (83.3%) and contralateral in 1 (16.7%). In 2 (8.7%) of the metachronous cases, BC was diagnosed before GM, with intervals ranging from 2 to 3 years after completion of BC treatment. All patients in this subgroup were premenopausal. In 1 (50.0%), GM developed in the contralateral breast three years after radical mastectomy. Another patient, 1 (50.0%), developed GM two years after completion of BC treatment, presenting with contralateral breast pain and a mass-like lesion (Tables 2 & 4).
Management of GM was heterogeneous: conservative treatment (antibiotics, NSAIDs, corticosteroids, methotrexate) alone in 8 (34.8%) of all cases, surgical intervention alone in 3 (13.0%), and mixed approaches in 12 (52.2%). For BC, mastectomy was performed in 11 (47.8%) of cases, breast-conserving surgery in 9 (39.1%). Neoadjuvant chemotherapy was used in 7 (30.4%), adjuvant chemotherapy in 6 (26.1%), hormone therapy in 9 (39.1%), and radiotherapy in 8 (34.8%). Follow-up duration ranged from 2 to 53 months (Tables 2 & 5).
|
Author (year) [ref] |
Management of GM |
Management of BC |
Follow-up duration |
|
Salih et al., 2025 [2] |
AB, ibuprofen, mastectomy + reconstruction |
WLE, mastectomy + reconstruction, adjuvant CT (Docetaxel, Carboplatin), trastuzumab, ET |
N/A |
|
Freitas et al., 2020 [20] |
AB |
NAC, BCS, SLNB, ET |
53m |
|
Zavieh et al., 2024 [8]
|
Naproxen, open drainage |
NAC, mastectomy + reconstruction, RT, anti-HER2 therapy, ET |
N/A |
|
Corticosteroids |
NAC, mastectomy, SLNB, RT |
N/A |
|
|
Corticosteroids |
NAC, BCS, SLNB, RT |
|
|
|
Zhu et al., 2024 [18]
|
Anti-inflammatory therapy, mirabilite compress, WLE |
BCS, SLNB |
N/A |
|
Anti-inflammatory therapy, aspiration, WLE |
BCS, SLNB |
N/A |
|
|
Aspiration, WLE |
BCS, SLNB |
N/A |
|
|
Oddó et al., 2019 [6] |
AB, steroids, MTX, multiple drainages, mastectomy |
Lumpectomy, total mastectomy |
>4m |
|
Tavakol et al., 2022 [9] |
Prednisolone, hydroxychloroquine |
Observation/surveillance |
12m |
|
Yoshida et al., 2023 [4] |
Prednisolone, total mastectomy |
Excision, total mastectomy, ET |
18m |
|
Zangouri et al., 2022 [22] |
Prednisolone, MTX |
N/A |
N/A |
|
Çalış and Kilitçi, 2018 [19] |
MRM |
MRM, ALND, adjuvant CT |
N/A |
|
Xie et al., 2022 [23] |
Rifampicin (6 months), BCS |
BCS, ALND, RT, ET, adjuvant CT |
N/A |
|
Evans et al., 2021 [17] |
AB, surgical drainage |
Oncoplastic WLE, SLNB, ALND, adjuvant CT, RT, ET |
N/A |
|
Salih et al., 2023 [16] |
Steroids, MTX, simple mastectomy |
Simple mastectomy, SLNB, ET |
6m |
|
Mazlan et al., 2012 [24] |
Repeated drainages, prednisolone |
Craniotomy and orbital decompression (metastatic disease) |
6m |
|
Chen et al., 2025 [21] |
Two surgical resections |
Mastectomy, ALND, adjuvant CT |
36m |
|
AkbariRad et al., 2025 [7] |
Prednisone, MTX |
NAC, mastectomy, RT, ET |
N/A |
|
Limaiem et al., 2013 [10] |
Radical mastectomy |
Radical mastectomy, ALND |
2m |
|
Özşen et al., 2018 [14] |
Steroids, surgical excision |
Surgical excision |
N/A |
|
Mahmood et al., 2025 [5] |
NSAIDs, steroids, MTX |
NAC, MRM, adjuvant CT, RT |
N/A |
|
Kaviani et al., 2017 [15] |
Observation |
NAC*, BCS, SLNB, RT, ET |
N/A |
|
Abbreviation. Ref: reference; AB: antibiotics; ALND: axillary lymph node dissection; BCS: breast-conserving surgery; GM: granulomatous mastitis; BC: breast cancer; CT: chemotherapy; ET: endocrine therapy; HER2: human epidermal growth factor receptor 2; MRM: modified radical mastectomy; MTX: methotrexate; NAC: neoadjuvant chemotherapy; NSAIDs: non-steroidal anti-inflammatory drugs; RT: radiotherapy; SLNB: sentinel lymph node biopsy; WLE: wide local excision; N/A: not available. *Neoadjuvant Chemotherapy was primarily for the BC, which incidentally aided the resolution of the observed GM mass as well. |
|||
Discussion
It is estimated that approximately 25% of all cancers, including those of the colon, esophagus, stomach, and liver, arise in the setting of chronic inflammation or infection; yet the extent to which this paradigm applies to breast cancer remains uncertain [14]. Because GM produces chronic inflammation within the breast, the coexisting GM and BC cases in this review provide a direct clinical setting in which this question can be examined. Whether the granulomatous response in these cases represents a sarcoid-like reaction to an underlying carcinoma, or whether chronic GM-related inflammation contributes to malignant transformation, remains the central unresolved question that the present findings can help inform [7,10]. In a previous literature review of patients with lobular GM and BC, cases were categorized as GM preceding cancer (45%), concurrent with cancer (45%), and following cancer (10%) [7]. The present analysis shows a higher proportion of synchronous cases (65.2%) and a lower proportion of GM first cases (26.1%). The median age of 40 years reported by that same review aligns closely with the median age of 42 years in this analysis, and both reviews found a predominance of premenopausal women (approximately 75% in both) [7].
The most common presenting symptoms in the present review were palpable breast mass, pain, swelling, erythema, and abscess formation. A previous review reported similar symptoms: palpable mass (100%), swelling (78%), pain (56%), erythema (33%), and abscess (33%) in patients with GM preceding BC [7]. Salih et al. reported a 30-year-old woman who presented with left breast pain for seven days, along with a large palpable lump and axillary lymphadenopathy, initially diagnosed as recurrent GM after a previous episode [16]. Evans et al. noted a distracting presentation of GM in one breast that delayed investigation of contralateral BC, highlighting that GM can be the dominant clinical feature even when malignancy is present elsewhere [17]. Regarding imaging findings, this review found that mammography commonly showed asymmetric density, focal opacity, and calcification. Reported calcification patterns included dense calcification resembling gravel, microcalcifications, focal asymmetric opacity with calcifications, and operative bed deformity with skin thickening [16,18,19]. In contrast, one report described diffuse dense breasts with focal areas of higher density but no evident microcalcifications [6]. On ultrasound, the current review identified irregular hypoechoic areas, skin thickening, ductal dilatation, and fluid collections; additional reports described a heterogeneous area with fluid echogenicity and moderate surrounding edema [2], as well as a BI-RADS 4c lesion with a new palpable area developing during chemotherapy [20]. On MRI, the current review noted non-mass enhancement, rim enhancement, and washout kinetic curves. Reported MRI findings in individual cases included a widespread T2-weighted high-signal lesion with a fast washout pattern and pre-spectral edema (classified as BI-RADS 4B initially and 4A after treatment) [4]; posterior edema of the glandular layer with ductal dilatation [18]; and a clumped focal non-mass-like enhancement with additional heterogeneous non-mass-like enhancement in the surgical bed, classified as MR-4 [16].
The role of core needle biopsy (CNB) in diagnosing coexisting GM and BC remains a subject of debate within the included cases. On one hand, CNB proved sufficient for diagnosing GM in nine (39.1%) and BC in 14 (60.9%) of cases, supporting its use as a first-line sampling tool. Several included cases reached definitive dual diagnoses through CNB alone, suggesting that when adequately targeted, CNB can successfully identify both conditions [2,7,9,18]. On the other hand, excisional or incisional biopsy was ultimately required in 30.4% of GM cases and 21.7% of BC cases, pointing to the inherent sampling limitations of CNB in an inflamed, heterogeneous breast. In some reports, DCIS was identified only after excisional surgery: in one patient, excision followed failure of medical GM therapy; in another, residual post-treatment imaging abnormalities prompted excision after CNB had initially confirmed GM alone [4,14]. Taken together, these findings suggest that while CNB is a reasonable and often adequate initial approach, its diagnostic yield in the setting of GM-associated malignancy is inconsistent, and a low threshold for escalation to excisional sampling should be maintained, particularly in refractory or recurrent cases.
Management of GM across the included cases was notably heterogeneous, reflecting the absence of a standardized treatment protocol for this condition. This variability is consistent with the review of AkbariRad et al. who reported that among patients who developed GM before BC, initial GM therapy included systemic corticosteroids alone in 40%, combined with methotrexate in 30%, incision and drainage in 20%, and antibiotics in 10%, with complete resolution requiring a median of 18 months [7]. Several cases in the present review illustrate the refractory nature of GM in this context. Mahmood et al. described a stepwise escalation from NSAIDs to prednisolone and ultimately methotrexate before GM was controlled [5], and Chen et al. required two surgical resections for GM that persisted in the contralateral breast of a BC survivor [21]. Among the three GM cases reported by Zavieh et al., one was managed with naproxen and open drainage, and the other two with corticosteroids alone [8].
The coexistence of GM complicated BC management in several cases. One report described a new palpable area emerging during neoadjuvant chemotherapy that initially raised concern for tumor progression but was ultimately attributed to GM [20], and Mahmood et al. reported GM onset during the second cycle of chemotherapy for BC, necessitating concurrent management of both conditions [5]. These findings highlight that when GM and BC coexist, treatment planning must account for both conditions simultaneously, as the inflammatory process can obscure tumor response assessment and complicate surgical decision-making.
Our review has several limitations. First, it relied exclusively on case reports and small case series. Second, incomplete reporting of key variables (e.g., parity, lactation, follow-up) precluded subgroup analyses. Third, most cases originated from Iran and China, limiting generalizability.
Conclusion
Granulomatous mastitis and BC can coexist synchronously or metachronously, and overlapping imaging features together with the limitations of core needle biopsy frequently delay the diagnosis of malignancy. Clinicians should maintain a low threshold for repeat biopsy or excisional sampling whenever GM fails to respond to standard therapy or recurs.
Declarations
Conflicts of interest: The authors have no conflicts of interest to disclose.
Ethical approval: Not applicable.
Consent for participation: Not applicable.
Consent for publication: Not applicable.
Funding: The present study received no financial support.
Acknowledgements: None to be declared.
Authors' contributions: BAA, ZDH and LLH: Major contributors to the conception of the study, as well as the literature search for related studies, and manuscript writing. DJHR, SJH, ADA, SMA, STL: Literature review, critical revision of the manuscript, and processing of the tables. HAS, SSA, GMF, DKA: Data extraction, data organization, and critical revision. All authors have read and approved the final version of the manuscript.
Use of AI: Claude Opus 4.8 was used to assist with language refinement and improve the overall clarity of the manuscript. All content was thoroughly reviewed and approved by the authors, who bear full responsibility for the final version.
Data availability statement: Not applicable.
References
- Salih AM, Pshtiwan LR, Latif S, Ali HO, Abdullah AM, Baba HO, et al. Granulomatous mastitis in accessory breast tissue: A rare presentation and surgical management. Biomedical Reports. 2024;20(4):1-4. doi:10.3892/br.2024.1750
- Salih AM, Latif S, Ali RM, Pshtiwan LR, Ali HO, Abdullah AM, et al. Granulomatous mastitis co-existing with breast cancer: A case report and mini-review of the literature. World Academy of Sciences Journal. 2025;7(6):101.doi:10.3892/wasj.2025.389
- Esmaeil NK, Salih AM, Hammood ZD, Pshtiwan LR, Abdullah AM, Kakamad FH, et al. Clinical, microbiological, immunological and hormonal profiles of patients with granulomatous mastitis. Biomedical Reports. 2023;18(6):41. doi:10.3892/br.2023.1624
- Yoshida N, Nakatsubo M, Yoshino R, Ito A, Ujiie N, Yuzawa S, et al. Concurrent granulomatous mastitis and ductal carcinoma in situ. Cureus. 2023;15(5): cureus.38377. doi:10.7759/cureus.38377
- Mahmood A, Idrees R, Vohra LM. Concurrence of idiopathic granulomatous mastitis and breast cancer in a patient on neoadjuvant chemotherapy: a case report. International Journal of Surgery Case Reports. 2025;126:110702. doi:10.1016/j.ijscr.2024.110702
- Oddó D, Domínguez F, Gómez N, Méndez GP, Navarro ME. Granulomatous lobular mastitis associated with ductal carcinoma in situ of the breast. SAGE open medical case reports. 2019;7:2050313X19836583. doi:10.1177/2050313X19836583
- AkbariRad M, Sheybani F, Gharib M, Aghel E, Emadzadeh M, Mottaghi M. Coexistence of lobular granulomatous mastitis and breast cancer: Case report and case-based literature review. International Journal of Surgery Case Reports. 2025;133(C):111628. doi:10.1016/j.ijscr.2025.111628
- Zavieh MM, Omranipour R, Alipour S, Sarkardeh M. Idiopathic Granulomatous Mastitis and Breast Cancer: Three Cases and Review of 16 Previous Cases. Acta Medica Iranica. 2024;61:378-80. doi:10.18502/acta.v62i6.18238
- Tavakol M, Alvand S, Ardalan FA, Assarian A. Idiopathic granulomatous mastitis with incidental lobular carcinoma in situ: A case report: IGM with LCIS. Archives of Breast Cancer. 2022;9(3-SI):315-9. doi:10.32768/abc.202293SI315-319
- Limaiem F, Khadhar A, Hassan F, Bouraoui S, Lahmar A, Mzabi S. Coexistence of lobular granulomatous mastitis and ductal carcinoma: a fortuitous association?. Pathologica. 2013;105(6):357-60.
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. bmj. 2021;372:n71. doi:10.1136/bmj.n71
- Kakamad FH, Mohammed SH, Abdalla BA, Hussein DA, Hammood ZD, Kakamad SH, et al. Non-Recommended Publishing Lists: Strategies for Detecting Deceitful Journals. Barw Medical Journal. 2026;4(1):13-21. doi:10.58742/bmj.v4i1.227
- Freire MV, Thissen R, Martin M, Fasquelle C, Helou L, Durkin K, et al. Genetic evaluation of patients with multiple primary cancers. Oncology Letters. 2024;29(1):4. doi:10.3892/ol.2024.14750
- Özşen M, Tolunay Ş, Gökgöz MŞ. Case report: ductal carcinoma in situ within a granulomatous mastitis. European journal of breast health. 2018;14(3):186. doi:0.5152/ejbh.2018.3894
- Kaviani A, Zand S, Karbaksh M, Ardalan FA. Synchronous idiopathic granulomatosis mastitis and breast cancer: a case report and review of literature. Arch Breast Cancer. 2017;4(1):32-6. doi:10.19187/abc.20174132-36
- Salih AM, Pshtiwan LR, Abdullah AM, Dhahir HM, Ali HO, Muhialdeen AS, et al. Granulomatous mastitis masking ductal carcinoma in situ: A case report with literature review. Biomedical Reports. 2023;20(2):17. doi:10.3892/br.2023.1705
- Evans J, Sisk L, Chi K, Brown S, To H. Concurrent granulomatous mastitis and invasive ductal cancer in contralateral breasts—a case report and review. Journal of Surgical Case Reports. 2021;2021(12):rjab519. doi:10.1093/jscr/rjab519
- Zhu J, Miao X, Li X, Zhang Y, Lou Y, Chen H, et al. Granulomatous lobular mastitis co-existing with ductal carcinoma in situ: Report of three cases and review of the literature. Annals of Diagnostic Pathology. 2024;68:152241. doi:10.1016/j.anndiagpath.2023.152241
- Çalış H, Kilitçi A. Granulomatous mastitis concurrence with breast cancer. European Journal of Breast Health. 2018;14(1):58. doi:10.5152/ejbh.2017.3804
- de Freitas JR, de Souza MF, Lopes M, Bitencourt L, Athanazio DA. Cystic neutrophilic granulomatous mastitis during chemotherapy treatment for invasive breast carcinoma–a rare lesion that simulates tumor progression. Surgical and Experimental Pathology. 2020;3(1):23. doi:10.1186/s42047-020-00075-y
- Chen J, Zhang B, Zhou T. Recurrent Granulomatous Mastitis in the Contralateral Breast Following Radical Mastectomy for Breast Cancer: A Case Report and Literature Review. BMC Women's Health. 2025;25(1):464. doi:10.1186/s12905-025-03971-1
- Zangouri V, Niazkar HR, Nasrollahi H, Homapour F, Ranjbar A, Seyyedi MS. Benign or premalignant? Idiopathic granulomatous mastitis later diagnosed as ductal carcinoma breast cancer: Case report and review of literature. Clinical Case Reports. 2022;10(9):e6323. doi:10.1002/ccr3.6323
- Xie S, Yu H, Gao H, Lian Z, Wang Q. Breast cancer coexisting with granulomatous mastitis in a young woman. British Journal of Hospital Medicine. 2022;83(6):1-3. doi:10.12968/hmed.2021.0426
- Mazlan L, Niza AS, Jaszle JS, Harlina ML, Sellymiah A, Rohaizak M. Breast carcinoma occurring from chronic granulomatous mastitis. The Malaysian Journal of Medical Sciences: MJMS. 2012;19(2):82

Copyright (c) 2026 The Author(s)

This work is licensed under a Creative Commons Attribution 4.0 International License.